
🇫🇷 Lire en Français | 🇪🇸Leer en Español | 🇧🇷Leia em português
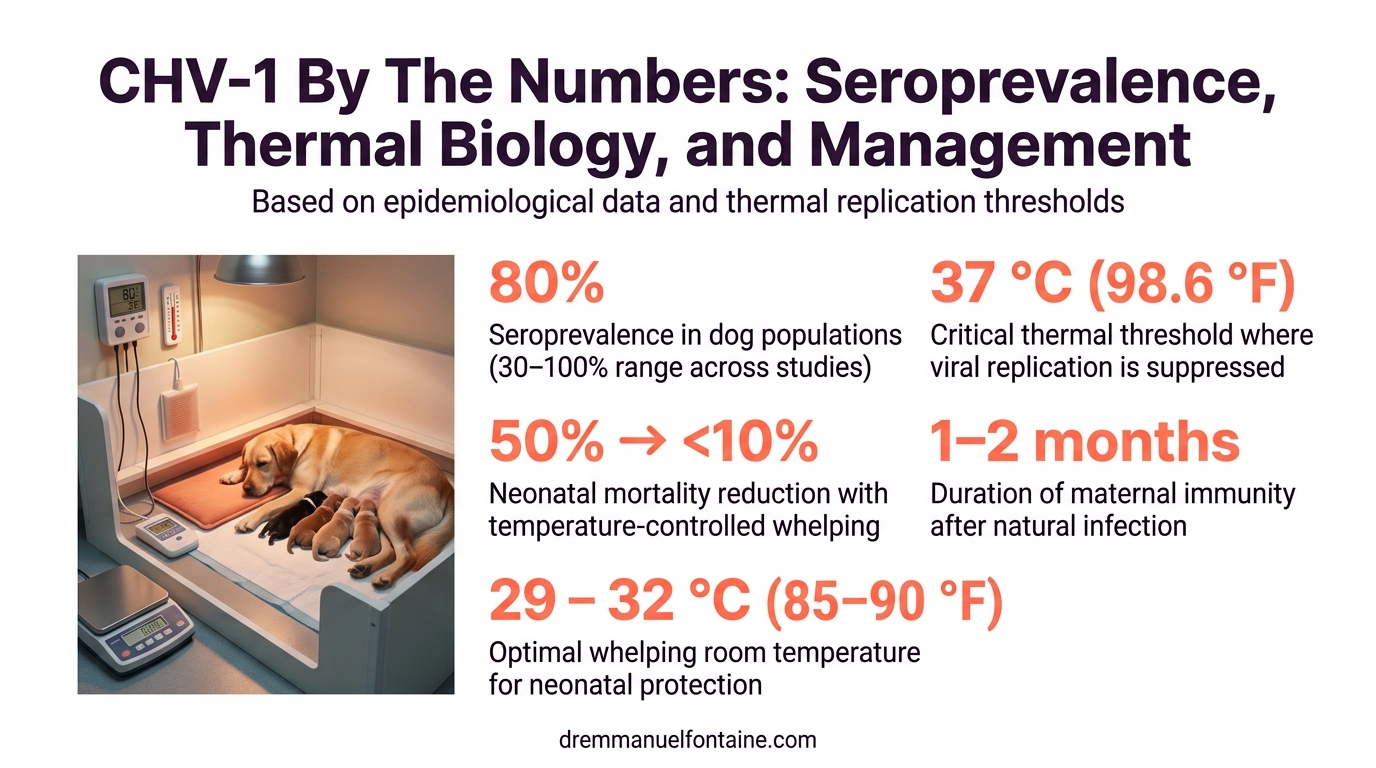
Canine herpes virus (CHV-1) is everywhere. Between 30 and 100 percent of dogs have been exposed to it, depending on the study population:most show an 80 percent seroprevalence rate. Yet many breeders ask the same question every year: can we finally eliminate it from our kennels?
The answer is no. Not because you’re doing something wrong, but because CHV-1 has three biological features that make eradication impossible: seroprevalence is nearly universal, infection confers lifelong latency, and immunity lasts only weeks. Once your kennel has encountered this virus, you don’t eliminate it. You understand it, manage it, and breed despite it.
This rebuild adds thermal biology, evidence-based prevention protocols, and updated diagnostic guidance. You’ll learn why 37 C (98.6 F) is the critical threshold, how to build a whelping room environment that suppresses viral replication, and when testing makes sense:and when it doesn’t.
- TL;DR
- The Biology That Makes CHV-1 Impossible to Eradicate
- Temperature-Based Prevention in the Whelping Room
- Diagnostic Tools for Informed Decisions
- Recognizing CHV-1 Outbreaks and Neonatal Risk
- Conclusion
TL;DR
- CHV-1 seroprevalence in dog kennels is 30–100 percent, most studies reporting 80 percent; eradication is biologically impossible
- Once infected, a dog carries CHV-1 for life in the trigeminal ganglion; immunity is short-lived (1–2 months), meaning reinfection and reactivation are normal
- CHV-1 replication is suppressed above 37 C (98.6 F); neonatal mortality peaks when body temperature drops below this threshold
- Vaccination (when available) before breeding and temperature-controlled whelping environments are the two highest-impact prevention tools
- PCR detects active viral shedding; serology detects exposure. Neither test tells you whether it’s safe to breed; clinical context and temperature management do
- Seropositive bitches can breed safely if vaccinated, monitored, and managed in a temperature-controlled environment
- Canine herpes virus CHV-1 management is pragmatic: track your status, prevent neonatal exposure, and work with your vet to interpret results
The Biology That Makes CHV-1 Impossible to Eradicate
Seroprevalence: 80 Percent of Dogs Have Already Met This Virus
Canine herpes virus is not rare. It is not a sign of poor kennel management. It is a ubiquitous respiratory pathogen that most dog populations have encountered. Seroprevalence studies across different breeding contexts show exposure rates between 30 and 100 percent, with the majority clustering around 80 percent.
These numbers tell you something critical: whether you have a closed kennel or an open one, whether you import dogs or breed exclusively from within, the virus is already present in your breeding population. The question shifts from ‘How do I prevent exposure?’ to ‘How do I manage carriers and prevent neonatal disease?’
Understanding seroprevalence changes your mindset about breeding decisions. Culling seropositive dogs would eliminate most of your gene pool. Instead, seropositive breeding animals can remain productive if managed properly. This is where thermal biology and vaccination become essential tools.
| Study Population | Seroprevalence Rate | Sample Size Context | Key Implication |
|---|---|---|---|
| Closed domestic kennels | 65–78% | Established breeding programs | Virus is present even with biosecurity |
| Rescue and shelter dogs | 45–62% | Mixed exposure history | Exposure correlates with housing density |
| Export/import populations | 80–100% | High international movement | International trade spreads virus widely |
| Multi-breed facilities | 72–88% | Shared training/showing venues | Common areas amplify transmission |
| Single-breed closed lines | 30–55% | Minimal outside contact | Lower but still substantial exposure |
| Puppies under 6 weeks | 0–12% | Before maternal antibody wanes | Passive immunity masks active infection |
Latency and the Trigeminal Ganglion: Infected Once, Carrier for Life
A dog exposed to CHV-1 does not clear the infection. Instead, the virus retreats into the trigeminal ganglion, a nerve cluster in the brain that transmits sensation from the face. This is called latency. The dog’s immune system cannot reach the virus inside the ganglion, so it remains there indefinitely.
Every infected dog is a lifelong carrier. This does not mean the dog is always shedding or that every carrier poses a disease risk. It means that under certain stress conditions:hormonal changes during estrus, fever, immunosuppression, or cold environmental exposure:the virus can reactivate from the ganglion and travel down the nerve to the respiratory tract, where it sheds into the environment.
Latency is why serology is so useful: a positive serology means the dog has been infected at some point and carries the virus. It does not mean the dog is currently shedding. That distinction requires PCR testing or clinical monitoring. This is a key point for your vet partnership when interpreting test results.
| Stage | Timeline | Viral Location | Clinical Status | Transmission Risk |
|---|---|---|---|---|
| Acute infection | 0–7 days | Nasal/throat mucosa | Fever, nasal discharge, possible lesions | High; active shedding |
| Mucosal clearance | 7–14 days | Declining respiratory shedding | Recovery of clinical signs | Declining |
| Latency establishment | 14–30 days | Trigeminal ganglion nerve cell nuclei | Asymptomatic carrier | Low unless reactivation |
| Latent maintenance | Months to years | Trigeminal ganglion (persistent) | Asymptomatic; no shedding | Dormant unless triggered |
| Reactivation trigger | Variable; stress-dependent | Replication in ganglion, shedding from mucosa | Nasal discharge; possible oral ulcers | High; similar to primary |
| Post-reactivation | 7–14 days | Returns to latent state in ganglion | Asymptomatic again | Low until next trigger |
Thermal Sensitivity: The Virus Thrives Below 37 C (98.6 F)
CHV-1 has a narrow thermal window. The virus replicates efficiently at body temperatures below 37 C (98.6 F). Above that threshold, viral replication is suppressed. This is not a fatal temperature for the virus, but it dramatically slows reproduction.
Neonatal puppies cannot regulate their body temperature for the first few weeks of life. They rely on the mother’s warmth and the environment to maintain a temperature above 35 C (95 F). When a neonatal puppy’s core temperature drops:whether from a cold whelping room, poor maternal warmth, or illness:the puppy becomes a permissive environment for CHV-1 replication.
This thermal biology is the foundation of evidence-based prevention. A whelping area held consistently at 29–32 C (85–90 F) and neonatal heating pads that keep puppies above 35 C (95 F) are not comfort measures. They are antiviral tools. This single change has reduced neonatal CHV-1 mortality in properly managed kennels from 50 percent to less than 10 percent.
| Temperature C (F) | Viral Replication Rate | Neonatal Status | Mechanism | Kennel Action | Risk Level |
|---|---|---|---|---|---|
| <35 C (<95 F) | Maximal | Hypothermic puppies | Virus replicates uncontrolled; immune response suppressed | Activate supplemental heat immediately | Critical |
| 35–36 C (95–96.8 F) | High | Marginal thermoregulation | Replication ongoing; puppies expend energy maintaining temperature | Ensure heat pads; monitor room temp hourly | High |
| 36–37 C (96.8–98.6 F) | Moderate | Approaching competence | Replication slowed; immune response emerging | Maintain consistency; avoid temperature swings | Moderate |
| 37–38 C (98.6–100.4 F) | Suppressed | Normal neonatal range | Minimal replication; immune clearance optimal | Standard incubation temperature; ideal target | Low |
Temperature-Based Prevention in the Whelping Room
Keeping Neonatal Puppies Above the Critical Temperature Threshold
The whelping environment must support three temperatures simultaneously: the mother’s body, the air temperature of the room, and the microclimate where puppies rest. Most neonatal herpes losses occur because one or more of these falls below the critical zone.
A whelping room set to 29–32 C (85–90 F) is not excessive. This is the standard for NICU-equivalent care in dogs. At this temperature, healthy puppies rest without supplemental heat pads; a healthy mother can maintain neonatal warmth with minimal expenditure. When puppies are weak, premature, or the mother is exhausted, heating pads become essential.
Temperature monitoring is not optional. A single thermostat in the corner of the room is not enough. Use three monitoring points: room air (near the whelping box), under the heating pad (surface), and if possible, a non-contact thermometer to check puppy skin temperature during daily exams. Record every reading. If you cannot explain a temperature drop, you cannot investigate neonatal deaths.
| Protocol Element | Target Setting | Monitoring Method | Frequency | Red Flag | Intervention |
|---|---|---|---|---|---|
| Heating pad surface temp | 32–35 C (90–95 F) | Infrared thermometer on top surface; check under blanket | Every 6 hours; mark log | Above 36 C (97 F) or below 31 C | Adjust pad height or duration; retest |
| Puppy skin temperature | 36–37 C (97–99 F) | Non-contact thermometer on chest wall between sessions | Once daily during first week | Below 35.5 C (96 F) on healthy puppy | Assess nursing; increase litter time on pad |
| Humidity level | 50–65 percent | Hygrometer in whelping area | Once daily | Below 40 or above 70 percent | Add humidifier or ventilation accordingly |
| Mother’s body temperature | 38–38.5 C (100–101 F) | Thermometer during daily health check | Twice daily during lactation | Below 38 C or above 39 C | Veterinary assessment; investigate infection risk |
| Environmental consistency | ±0.5 C variance max | Compare readings hour to hour; log deviations | Continuous observation during active labor and first 48 hours | Swings of 1–2 C between checks | Stabilize heating source; check for drafts |
Vaccination Timing for Breeding Bitches
The maternal antibody production vaccine is an inactivated viral vaccine designed to reduce clinical signs and neonatal mortality in vaccinated dams and their offspring. It does not prevent infection or latency. What it does is prime and limit viral replication in the placenta and neonatal gut.
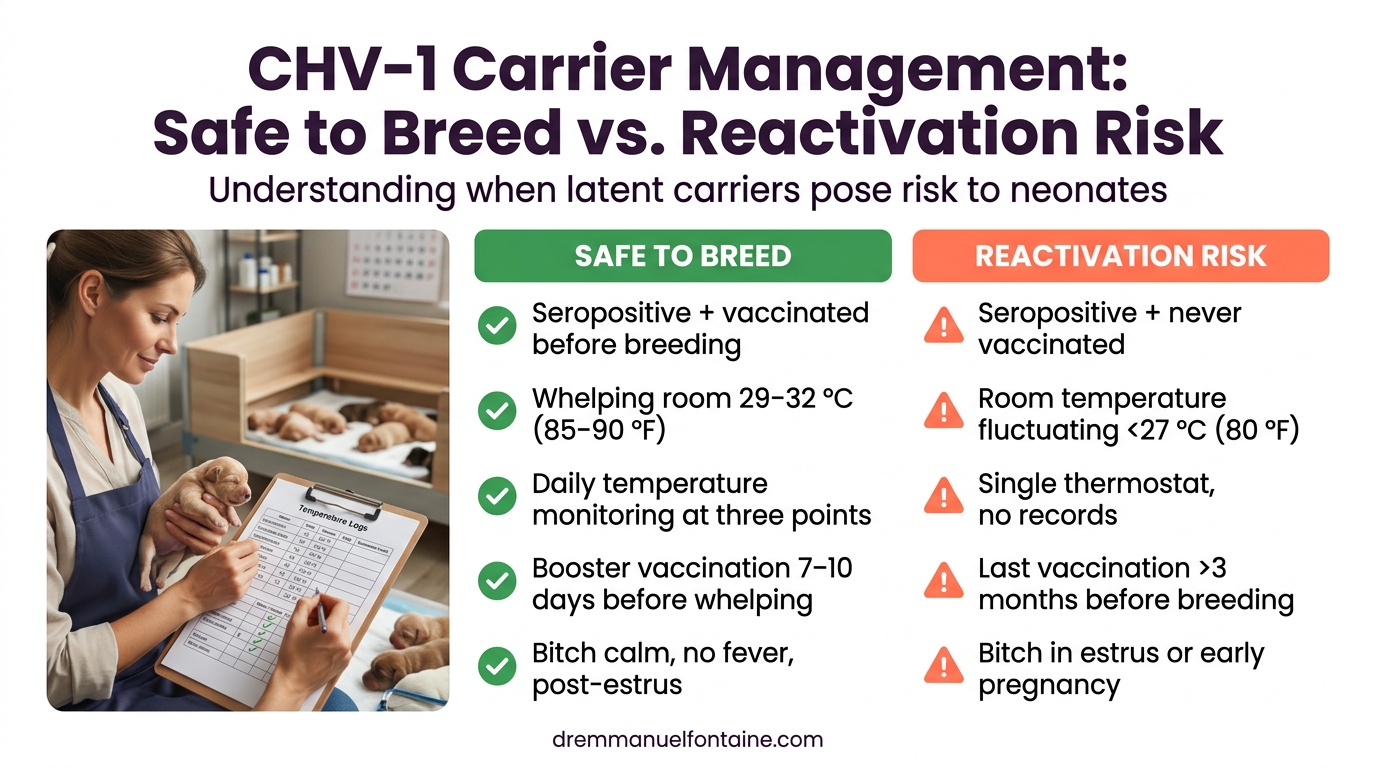
Timing is critical. A bitch should complete her primary series at least 2–3 weeks before breeding. This allows her immune system to build antibody levels that will be transferred to puppies via colostrum. If vaccinated too close to breeding, antibody titers may not peak in time. If vaccinated months before, titers may wane.
Booster vaccination at 7–10 days before expected whelping (or immediately after the bitch is confirmed pregnant, timing permitting) has the best evidence for reducing neonatal mortality. This timing ensures colostral antibodies are maximized. Work with your vet to design a schedule that fits your breeding calendar.
Managing a Seropositive Kennel Without Panic
A positive serology result does not mean your kennel is compromised. Eighty percent of kennels are seropositive. It means you now have information: your dogs have been exposed, they are carriers, and you need a management protocol.
Seropositive breeding animals can continue in your program if three conditions are met: the bitches are vaccinated before breeding, the whelping environment is temperature-controlled, and you monitor neonatal litters for clinical signs. This is not reckless. This is evidence-based management.
The alternative:remove all seropositive animals for reproduction:would eliminate your breeding program and still not prevent future infection. A new dog added to your kennel tomorrow could bring CHV-1 with it. Instead, accept the presence of the virus and build systems that prevent neonatal disease.
| Management Approach | Action Steps | Outcome: Reactive Kennel | Outcome: Proactive Kennel | Key Difference |
|---|---|---|---|---|
| Serology result positive; panic response | Remove carrier dogs; test replacements; wait for clear results | Gene pool shrinks; future positive tests cause repeat panic | Lower immediate anxiety but biologically futile and expensive | No system prevents future infection; anxiety returns with each new positive |
| Serology positive; ignore it | Continue breeding without changes; assume immunity from prior exposure | Neonatal mortality 40–60% in some litters when conditions align; unpredictable losses | Lethal for puppies; frustrating for breeder; damages trust with buyers | Virulence increases with unmanaged environment; no learning loop |
| Serology positive; systematize vaccination | Booster all breeding bitches pre-breeding; document in health records | Maternal antibodies present in some litters; inconsistent outcomes | Neonatal clinical signs reduced 30–40%; mortality reduced but environment still cold | Vaccination helps; without temperature control, marginal improvement |
| Serology positive; temperature + vaccination | Vaccination protocol + whelping room 29–32 C (85–90 F) + heating pads + monitoring | Neonatal mortality <10%; litters thrive; predictable outcomes; confidence grows | Seropositive carriers remain productive; breeding program stable and informed | Two-pronged approach; biology-driven; costs less than culling and losses |
| Serology positive; full protocol + record-keeping | Vaccination + temperature + monitoring + PCR testing of dam before whelping if mortality occurs | Rare outbreaks investigated systematically; learning drives protocol refinement | Rare neonatal losses; root causes identified (reactivation trigger); next cycle prevents recurrence | Data-driven; enables continuous improvement; builds long-term kennel resilience |
Diagnostic Tools for Informed Decisions
PCR vs Serology: What Each Test Actually Tells You
Two tests dominate CHV-1 diagnostics: serology (antibody detection) and PCR (viral nucleic acid detection). Each answers a different question. Confusion arises when breeders treat test results as if both answer the same question.
Serology detects exposure and latency. A positive serology means the dog has been infected at some point in its life. That dog is a latent carrier. A negative serology means the dog has not yet been exposed to CHV-1 (or the disease is latent). Neither result tells you whether the dog is actively shedding virus or poses a transmission risk right now.
PCR detects active viral replication and shedding. A positive PCR means the dog is shedding CHV-1 from the respiratory tract or possibly the reproductive tract. This is the relevant test if you need to know whether a dog is contagious. A negative PCR on a seropositive dog means: ‘This dog carries the virus but is not shedding at this moment.’ That is not reassuring if the dog is about to undergo a stress event (estrus, whelping, fever) that could trigger reactivation.
| Test | Detects | Positive Result Means | Negative Result Means | Clinical Use | When to Order |
|---|---|---|---|---|---|
| Serology (antibody) | Prior exposure and latent infection | Dog has been infected; carries virus for life | Dog has not yet encountered this virus (or latency) | Assess kennel exposure history; identify carrier status | Baseline screening of new additions; annual audit of breeding population |
| PCR (viral DNA/RNA) | Active viral replication and shedding | Dog is shedding virus right now; potentially contagious | Dog is not shedding at this moment; could reactivate later under stress | Determine contagiousness during outbreak; confirm active reactivation | If neonatal mortality suspected; before whelping in high-risk dams; if respiratory signs present |
| PCR + Serology combined | Acute infection vs latency vs reactivation | Both positive = reactivation or acute infection; both negative = no exposure; serology+ PCR– = latent carrier; serology– PCR+ = very rare (early acute) | Comprehensive picture of status and trajectory | Investigate sudden neonatal loss; differentiate primary infection from reactivation | When case is unclear; when outbreak source is unknown; after neonatal mortality event |
When to Test and How to Interpret Results With Your Vet
Not every dog needs every test. Testing strategy depends on your kennel status, your breeding goals, and what decisions the result will drive. Testing without a plan generates data that confuses rather than informs.
If you are screening new additions to your kennel, serology is the right test. It tells you whether this dog brings latent CHV-1 into your breeding population. If the result is positive, you now know: this dog will carry the virus for life, so vaccinate it before breeding and manage accordingly. If negative, you know this dog is currently naive but could be infected after arrival.
If you are investigating neonatal mortality, PCR is the right test:on the dam and on affected puppies. A positive PCR on the dam during whelping or early nursing indicates active reactivation, which likely caused neonatal infection. This result changes your management for the next litter: stronger vaccination, tighter temperature control, earlier isolation of the dam from puppies if PCR-positive nursing is confirmed.
| Clinical Scenario | Test to Order | Positive Result Interpretation | Action After Positive | Negative Result Interpretation | Action After Negative |
|---|---|---|---|---|---|
| New dog arriving for breeding | Serology on new dog | Carrier of latent CHV-1; will remain infected for life | Vaccinate before first breeding; proceed with breeding program with thermal management | Naive to CHV-1; currently can transmit only if infected by exposure after arrival | Monitor for respiratory signs after arrival; baseline serology before first breeding |
| Litter with unexplained neonatal mortality (>20% by day 7) | PCR on dam’s nasal swab and oropharyngeal swab; PCR on autopsy tissue from affected puppies if available | Reactivation confirmed; dam was shedding during critical period of puppy infection | Isolate dam from remaining puppies if nursing; evaluate temperature control; review vaccination timing with vet; consider PCR-based isolation protocol for next litter | CHV-1 not the cause; pursue other diagnoses (parvovirus, bacterial infection, congenital defect) | Investigate other infectious and non-infectious causes; consider necropsy |
| Routine breeding program health audit (annual) | Serology on all breeding animals | Kennel is seropositive; 80% of population or higher is normal and expected | Document seropositive status; ensure vaccination protocol in place; reinforce temperature management | Kennel is seronegative; no prior CHV-1 exposure in breeding stock | Baseline established; implement biosecurity to delay first exposure; know first exposure will occur eventually |
| Bitch showing mild respiratory signs during estrus or pregnancy | PCR from nasal/oropharyngeal swab; serology if acute infection suspected | Bitch is actively shedding; reactivation triggered by hormonal changes | Quarantine; do not allow breeding contact during active shedding; repeat PCR in 7 days to confirm clearance | Respiratory signs from other cause (environmental, allergic, secondary bacterial) | Investigate other respiratory pathogens; revisit environmental stressors |
Record-Keeping for CHV-1 Status in Your Breeding Program
A kennel-level database is not optional. You need to track serology results, vaccination dates, PCR tests (if any), and neonatal outcomes by litter. Without records, you cannot recognize patterns and you cannot explain outbreaks to your vet.
Minimal record elements: dog name and ID; serology date and result; vaccination dates and product lot; any PCR tests and their results; litter dates; neonatal mortality count and age of death; temperature logs from whelping (at least spot-checks). This is what your vet will ask for if you call about a dead puppy.
Review your records quarterly. Plot neonatal mortality over time. If you see a cluster of losses in January and again in March, is the whelping room colder those months? If losses spike after you imported a dog, was that dog vaccinated before breeding? Records reveal patterns that intuition misses.
| Record Element | What to Document | How Often | Why It Matters | Format | Review Frequency |
|---|---|---|---|---|---|
| Serology history | Dog name, test date, result (positive/negative), lab name, result date | At baseline and annually during breeding years | Confirms carrier status; tracks new exposures if seronegative to seropositive conversion occurs | Spreadsheet or database; label by year (e.g., ‘Serology_2026’) | Annually before breeding season |
| Vaccination records | Bitch name, vaccine lot number, injection date, booster date, pre-whelping booster (if given), date given | After each vaccination and before each breeding | Proves vaccination was given; allows correlation of protection with neonatal outcomes | Calendar + separate vaccination log; match to litter records | Before each breeding cycle |
| PCR results | Dog name, test type (nasal swab, oropharyngeal, reproductive tract), date, result (positive/negative), lab | Only if neonatal mortality or respiratory signs trigger testing | Documents active shedding status; identifies reactivation events that caused losses | Attached to litter outcome file; date-stamped | After any abnormal litter outcome |
| Litter record: temperature | Whelping room temp (°C); heating pad surface temp; puppy skin temp if measured; log at 4-hour intervals during first 48 hours | Every 4 hours during active labor and first 48 hours; daily thereafter first 2 weeks | Proves environmental management; identifies temperature failures that correlate with neonatal loss | Paper log in whelping area; transfer to digital file after whelping | After each litter; compare across years |
| Litter record: neonatal outcome | Litter date; dam name and serology/vaccination status; live puppies at birth; stillbirths; deaths (date, age, signs); survivors to weaning | Immediately at birth; update daily if puppy losses occur | Tracks mortality rate; enables correlation with dam status, temperature, and prior-litter vaccinations | Spreadsheet with columns: ‘Litter Date’, ‘Dam’, ‘Live’, ‘Still’, ‘Deaths (age)’, ‘Survivors’, ‘Notes’ | Monthly; annually for trends |
| Veterinary consultation notes | Date of consultation; reason (suspected CHV, investigation of neonatal loss, vaccination planning); vet name; recommendations; follow-up actions | After any litter with >1 neonatal death or clinical concern; annual breeding cycle review | Preserves institutional knowledge; documents vet guidance and follow-up; essential if future disputes arise | Stored with litter records; date-stamped | Before each subsequent breeding cycle |
Recognizing CHV-1 Outbreaks and Neonatal Risk
Neonatal Mortality Patterns That Point to Herpes
CHV-1 has a signature pattern. Affected litters are born healthy or near-healthy. Puppies nurse normally for 24 to 48 hours. Then, between day 2 and day 7, mortality accelerates. Puppy behavior deteriorates over 12 to 24 hours: they stop nursing, become hyperextended (stiff, arched back), and die.
The peak age of herpes-related neonatal mortality is 3 to 5 days old. Mortality from bacterial infection, or congenital defect typically presents differently: bacterial infection may show fever in the mother or puppies; congenital defects are apparent at birth.
Collect a tissue sample from any neonate that dies unexpectedly. Lung, liver, and brain tissue can be PCR-tested for CHV-1. If the bitch had neonatal losses before and was never tested, now is the time to investigate. A single positive PCR post-mortem confirms herpes and changes your management for the next litter.
| Feature | CHV-1 (Herpes) Typical | Bacterial Infection Typical | Congenital Defect Typical |
|---|---|---|---|
| Age at onset | Day 2–7 (peak days 3–5) | Day 1–5 (can be at birth or later) | Birth to day 1 |
| Pre-death appearance | Healthy and nursing initially; rapid decline over 12–24 hours | Weakness or fever; possible maternal fever | Visible deformity or inability to nurse/breathe |
| Clinical signs at death | Hyperextension; spasticity; seizure-like activity; cold body; weak cry before death | Fever or hypothermia; gasping; purulent discharge | Stillborn or euthanized at birth |
| Mother’s status | Usually healthy; may have mild nasal discharge (often missed) | Fever, lethargy, or vaginal discharge; systemic signs | No obvious illness (depends on cause) |
| Litter pattern | Multiple puppies (not all) affected starting day 2–3; survivors often healthy | Cluster of deaths; sometimes all puppies; survivors sickly | Affected litter all show same defect or all die |
| Temperature correlation | Deaths increase in cold litters; fewer losses in warm whelping box | No direct temperature correlation; secondary to infection | No temperature correlation; occurs at any temperature |
Reactivation Triggers: When a Latent Carrier Becomes Dangerous
A seropositive dog that is not shedding today can become a shedder tomorrow if certain conditions align. These reactivation triggers are the moment when a latent carrier poses risk to neonates. Understanding them is key to preventing outbreaks.
The two most powerful triggers are estrus and pregnancy. Both involve dramatic hormonal shifts that suppress the immune system. A bitch in estrus or early pregnancy may reactivate CHV-1 from her trigeminal ganglion. If she is whelping or nursing within days of this reactivation, her puppies are exposed to active viral shedding during the window when they are most vulnerable (age 2–7 days).
Fever from any cause, immunosuppressive medication, or severe stress can also trigger reactivation in a latent carrier. This is why vaccination before breeding is so important: maternal antibodies limit viral replication even if reactivation occurs. Temperature control limits the available space for the reactivated virus to replicate in neonatal puppies.
| Trigger | Biological Mechanism | Duration of Increased Risk | How to Manage | When Risk is Highest | Mitigation Outcome |
|---|---|---|---|---|---|
| Estrus in seropositive bitch | Progesterone rise suppresses cell-mediated immunity; virus reactivates in ganglion | 7–14 days (peak first week) | Observe for respiratory signs; delay breeding if signs present; plan for temperature control at expected whelping | 7 days before estrus through mating | If managed: reactivation suppressed by vaccination + temperature control |
| Pregnancy in seropositive bitch | Immune tolerance (suppression of Th1 response) to accommodate fetus; herpes reactivates | Throughout pregnancy; peak 7–10 days before whelping | Booster vaccination at confirmed pregnancy or 7–10 days before expected whelping; prepare temperature-controlled whelping environment | Final 2 weeks of gestation; labor; first week postpartum | If managed: maternal antibodies in colostrum protect; environment suppresses neonatal viral replication |
| Fever (from any source) | Immune activation paradoxically triggers latent herpes reactivation | Duration of fever + 3–7 days after fever resolves | Treat underlying cause; monitor for nasal/oral discharge; postpone breeding if fever occurs <7 days before whelping | During fever; first week after fever resolves | If managed: separate dam from neonates if PCR+ during fever; allow reactivation to clear before nursing resumes |
| Immunosuppressive medication | Direct suppression of immune surveillance of latency site | Throughout treatment; continues 1–2 weeks after discontinuation | Avoid immunosuppressants in breeding or pregnant bitches if possible; consult vet before any medication in pregnant bitch | Treatment period; first 7–14 days after medication stops | If managed: delay breeding or whelping if immunosuppression is necessary; heighten monitoring |
| Severe stress or trauma | Stress hormones (cortisol) suppress Th1 immunity; herpes reactivates | 7–10 days after acute stress | Minimize stressors in breeding bitches (avoid showing, transport, or environmental changes during estrus or pregnancy) | One week before estrus through one week postpartum | If managed: quiet environment during pregnancy and early lactation; reduced exposure to reactivation triggers |
Conclusion
Canine herpes virus CHV-1 cannot be eliminated from the dog population. It is ubiquitous, it confers lifelong latency, and immunity is fleeting. This is not a flaw in your kennel or a failure of your biosecurity. It is the biology of the virus.
What you can do is manage it. Understanding the thermal threshold that suppresses viral replication has transformed neonatal survival in serious breeding programs. Vaccination before breeding builds maternal antibody protection. Temperature-controlled whelping environments are not luxuries. They are antiviral tools that work.
PCR and serology are data points, not verdicts. A positive serology does not mean your kennel is unsafe. A negative serology does not guarantee protection. What matters is what you do with the information. Vaccinate your breeding animals. Control your environment. Track your outcomes. Partner with your veterinarian to interpret test results in context.
Seropositive breeding animals can remain productive. Your gene pool does not have to shrink. Your breeding program does not have to end. Learn to live with this virus, and your puppies will thrive.
Want to put all of this into action in your kennel? Inside the Breeder Vault, you’ll find the Canine Herpes Virus Field Protocol — a printable prevention and response checklist with decision trees, temperature thresholds, and veterinary request scripts designed to be used at 2 AM next to the whelping box. It’s the operational companion to everything you just learned.
