🇫🇷 Lire en Français | 🇪🇸Leer en Español | 🇧🇷Leia em português
When a breeding dog misses a heat cycle or loses a pregnancy, the first suspect is often the thyroid. The story repeats across breeding communities worldwide: a breeder watches for the signs of hypothyroidism and worries, “Is this why we failed?” The narrative is persistent because it contains a kernel of biological truth. Thyroid function does matter in reproduction. But the truth stops there.
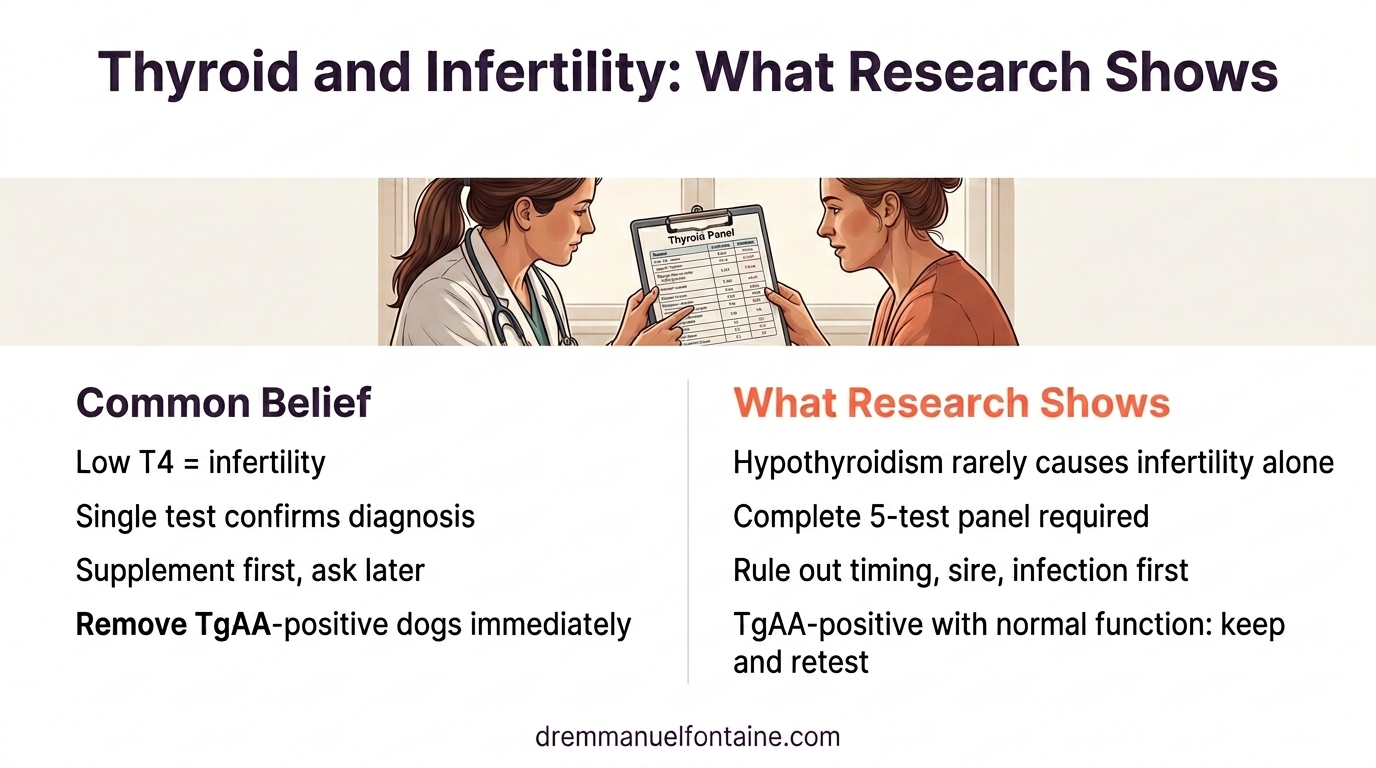
Here is what the science actually says: hypothyroidism is not a common cause of infertility in dogs. When hypothyroidism does cause reproductive failure, it is almost always accompanied by other obvious clinical signs, weight gain, lethargy, skin changes, that would lead you to consult your veterinarian long before fertility becomes the concern. If a dog shows no other symptoms, the chances of hypothyroidism being the cause of its reproductive problems are very low. This distinction matters. It is the difference between careful diagnosis and a leap of faith.
My role is to walk you through the evidence, show you how to distinguish between rigorous screening and false assumptions, and give you a framework that honors your experience while grounding your decisions in science. Hypothyroidism in breeding dogs is real. Overdiagnosis is also real. Here is where the two lines separate.
- TL;DR
- What you need to know about hypothyroidism and breeding
- What you need to do to screen properly
- What you need to have on file
- What you need to watch for
- Conclusion
TL;DR
- Hypothyroidism is not a common cause of infertility in dogs. When it does affect fertility, other clinical signs (weight gain, lethargy, skin problems) are almost always present. No other symptoms usually means the thyroid is not the problem.
- A single total T4 test (a basic screening blood test that measures the overall level of thyroid hormone circulating in the blood) is not enough to diagnose hypothyroidism. Demand a full panel from an approved laboratory.
- A test is only as good as its interpretation. Work with your veterinarian to understand the results, not just to get them.
- Rule out other causes of reproductive failure first: breeding timing, sire fertility, infectious disease status, and body condition are more likely culprits.
- A positive thyroglobulin autoantibody test does not mean removing the dog from the breeding program. If thyroid function is normal, keep the dog in your program and retest annually.
- If a dog is confirmed hypothyroid, the real question is: should it be bred at all? Only breed healthy animals, because breeding unhealthy ones propagates the problem to future generations.
What you need to know about hypothyroidism and breeding
Canine and human thyroid demands are not the same
Human pregnancies involve placental deiodinases and human chorionic gonadotropin (hCG), both of which amplify thyroid hormone demand. Dogs lack these mechanisms. Applying human thyroid literature to canine reproduction creates false assumptions about when supplementation is needed. This difference is fundamental to understanding why a hypothyroid human pregnant person might face real risks while a hypothyroid dog may not. Your veterinarian understands this distinction. You should too.
| Mechanism | Humans | Dogs |
|---|---|---|
| Placental deiodinases | Present, amplifies T4 to T3 | Absent |
| hCG production | High, thyrotropic activity | Not applicable |
| Metabolic demand increase | 20 to 40% above baseline | Minimal change |
| Clinical implication | Hypothyroidism poses higher risk | Risk is lower |
Hypothyroidism is not a common cause of infertility
This is the most important message in this article: hypothyroidism is not a common cause of infertility in breeding dogs. Scientific research reveals an uncomfortable truth for breeders who believe thyroid supplementation improves fertility. Naturally occurring hypothyroidism is only weakly tied to reproductive failure. Experimental studies show that a dog’s thyroid gland must be profoundly affected, essentially non-functional, before fertility problems manifest.
Even in deliberately induced hypothyroid dogs, interestrus intervals, conception rates, litter sizes, and gestation lengths remained normal. This evidence challenges the premise that minor thyroid imbalances drive reproductive failure.
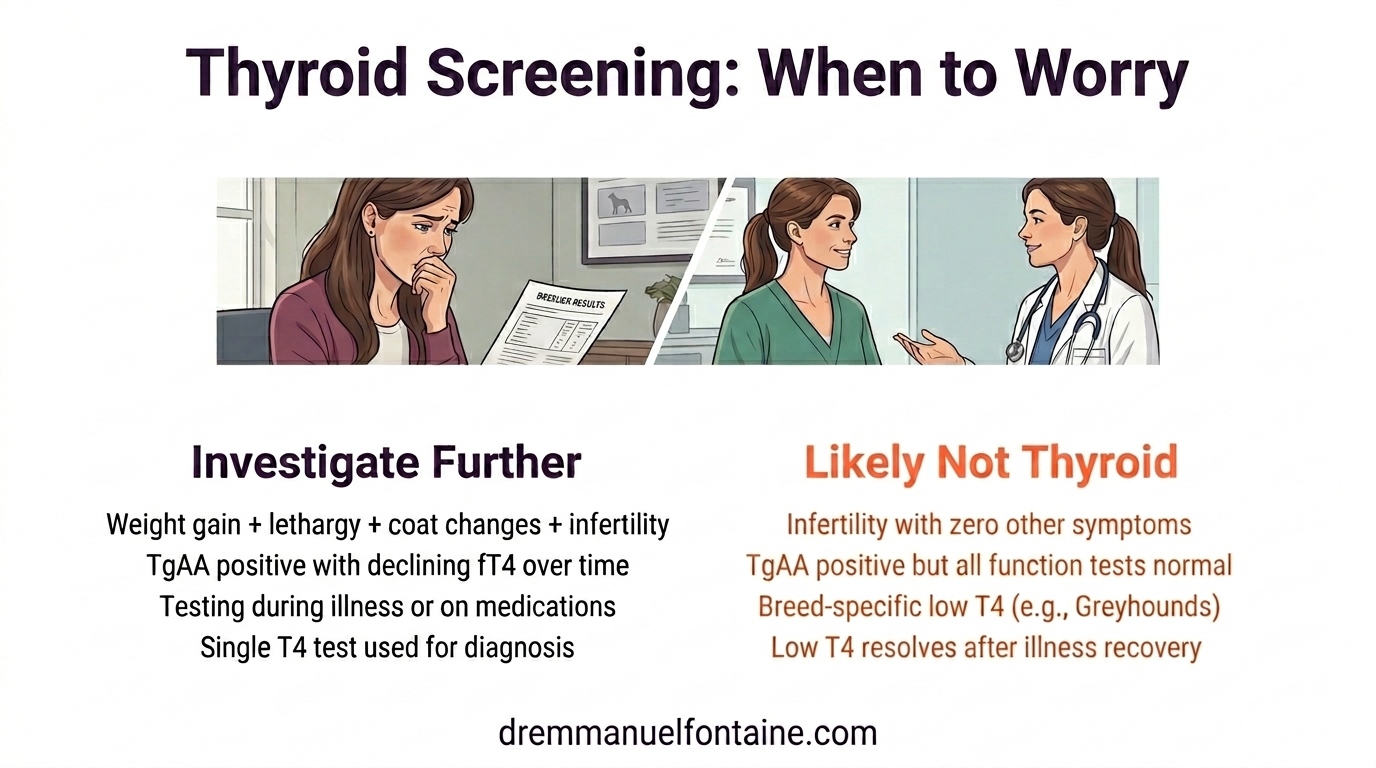
Here is the key: when hypothyroidism does cause infertility, there are usually other associated symptoms that lead to consultation, weight gain, lethargy, skin and coat changes, cold intolerance. If your dog shows none of these signs but is having reproductive difficulties, the thyroid is very unlikely to be the cause. Look elsewhere first.
| Study Context | T4 Status | Conception Rate | Litter Size | Gestation |
|---|---|---|---|---|
| Normal, untreated dogs | Normal | ~90% | 6 to 8 pups | 63 days |
| Experimentally hypothyroid | Low | ~88% | 6 to 7 pups | 63 days |
| Naturally hypothyroid (severe) | Very low | Variable | Often normal | 62 to 63 days |
Understanding thyroid tests: what they are and what they mean
Before discussing how to screen properly, you need to understand what these tests actually measure. Too often, test names are thrown around without explanation. Here is a plain-language guide to the five components of a complete thyroid panel.
Total T4 is the most basic thyroid blood test. It measures the overall level of thyroid hormone (thyroxine) circulating in the bloodstream. Think of it as a wide-angle snapshot: it captures everything, including thyroid hormone bound to proteins that is not actively doing anything. It is useful as a first screening tool, but on its own, it is not specific enough to confirm a diagnosis.
Free T4 by equilibrium dialysis (often written fT4ed) measures only the thyroid hormone that is unbound and biologically active, the portion your dog’s cells can actually use. This is the most reliable single marker for true hypothyroidism. The “equilibrium dialysis” part refers to the laboratory method used, which is more accurate than cheaper alternatives.
Canine TSH (thyroid-stimulating hormone) is produced by the pituitary gland in the brain. When thyroid hormone levels drop, the pituitary releases more TSH to try to stimulate the thyroid gland. A high TSH combined with low free T4 is a strong confirmation of primary hypothyroidism.
Thyroglobulin autoantibodies (TgAA) are markers of immune system involvement. When the immune system begins attacking the thyroid gland, these antibodies appear in the blood. A positive TgAA result does not mean clinical disease is present. It means the immune system has identified the thyroid as a target, and the dog has a higher risk of developing hypothyroidism over time.
T3 and free T3 (fT3) measure a secondary thyroid hormone called triiodothyronine. T3 is the more active form of thyroid hormone, converted from T4 in peripheral tissues. These tests round out the diagnostic picture, particularly in complex cases.
| Test | What It Measures | Plain-Language Summary |
|---|---|---|
| Total T4 | All circulating thyroxine (bound + free) | The wide-angle snapshot, good for initial screening |
| Free T4 (equilibrium dialysis) | Unbound, biologically active thyroxine | Best single marker of true thyroid status |
| Canine TSH | Pituitary response to thyroid levels | High TSH = the brain is telling the thyroid to work harder |
| Thyroglobulin autoantibodies (TgAA) | Immune markers against thyroid tissue | Positive = immune system is watching the thyroid |
| T3 / fT3 | Triiodothyronine (active hormone) | Completes the picture in complex cases |

Why a single T4 test misleads
Now that you know what these tests measure, you can see why relying on a single total T4 is a problem. Total T4 is sensitive but not specific. Non-thyroidal illnesses, medications, and breed-specific genetics can all lower circulating T4 without indicating hypothyroidism. A sick dog, a dog on glucocorticoids, or a healthy Greyhound may all show a low T4 on a quick screening test. This is called euthyroid-sick syndrome: the dog looks hypothyroid on paper but has a perfectly healthy thyroid.
Relying on this one number leads to false diagnosis and unnecessary medication. A proper diagnosis requires a full thyroid panel from an approved laboratory, not a snapshot from an in-house analyzer. This is where the partnership with your veterinarian matters most. A test is only as good as its interpretation.
| Factor | Effect on T4 | Actually Hypothyroid? |
|---|---|---|
| Non-thyroidal illness | Lowers T4 | No, usually not |
| Sulfonamides, steroids, phenobarbital | Lowers T4 | No, usually not |
| Breed genetics (sighthounds) | Lower baseline T4 | No, normal for breed |
| True hypothyroidism | Lowers T4 | Yes, confirmed by full panel |
| Euthyroid sick syndrome | Lowers T4 | No, resolves when illness resolves |
What you need to do to screen properly
Demand a complete thyroid panel, not a snapshot
The complete panel includes the five components described above: free T4 by equilibrium dialysis, total T4, canine TSH, thyroglobulin autoantibodies, and T3/fT3. Each answers a different question. Together, they tell the story. A single T4 tells you almost nothing.
When you talk to your veterinarian about screening, ask by name for these five tests. Be specific. And remember: the results need proper interpretation. Numbers on a page mean nothing without context, the dog’s breed, age, health status, and medication history all influence what those numbers mean. A test is only as good as its interpretation. This is where the partnership with your attending veterinarian is essential.
Each component of the panel answers a different diagnostic question. Free T4 by equilibrium dialysis is the best predictor of true hypothyroidism. Total T4 screens for non-thyroidal causes of low circulating hormone. Canine TSH confirms primary hypothyroidism by showing whether the pituitary is compensating. Thyroglobulin autoantibodies predict progression risk in dogs with normal function today. T3 and fT3 round out the picture in complex cases. Each of these tests was introduced in plain language in the earlier section, so you can match the lab number to the question it answers when results come back.
Establish a strict testing schedule
Begin screening around 1 year of age and repeat every 1 to 2 years while the dog is breeding, or until 8 to 10 years of age. Consistency matters. Timing also matters. Never test a dog that is currently ill or taking medications like sulfonamides, glucocorticoids, or phenobarbital. These interfere with results.
If your dog has been on medication or recently recovered from illness, work with your veterinarian to establish a washout period. Test when the dog is at its healthiest. This simple discipline prevents false positives that lead to unnecessary supplementation. Documentation is your ally here. Keep records of every test, date, laboratory, and result. Over time, trends emerge that a single number never reveals.
| Age / Status | Test Frequency | Key Condition |
|---|---|---|
| ~1 year (baseline) | Once at 12 months | Dog must be healthy |
| 1 to 8 years (breeding) | Every 1 to 2 years | No illness, no medications |
| 8 to 10 years (winding down) | Every 1 to 2 years if breeding | Continue screening if still active |
| Post-breeding (retired) | Optional, every 2 to 3 years | If monitoring for progression |
| Illness or medication use | Delay testing | Wait for recovery/washout |
Rule out other causes of reproductive failure
Before blaming the thyroid, work with your reproductive veterinarian to systematically rule out other common causes of infertility. Remember: hypothyroidism is not a common cause of infertility. If there are no other clinical signs pointing to thyroid disease, the answer is almost certainly somewhere else.
Check breeding timing. Verify sire fertility. Run infectious disease testing, including Brucella canis screening before every breeding. Conduct serial ultrasonography of the reproductive tract. Body condition matters too. A dog in poor body condition or with obesity faces reduced fertility independent of thyroid status. Your veterinarian can guide you through this systematic approach. As discussed in the earlier section on the weak association between hypothyroidism and infertility, the science shows that other factors often drive infertility more than thyroid problems do. The diagnostic pathway respects that reality.
| Diagnostic Step | What to Assess | Normal Finding |
|---|---|---|
| Breeding timing review | Cycle regularity and mating window | Cycle = 18 to 24 days, fertile window clear |
| Sire fertility evaluation | Sperm motility and morphology | Good motility, normal morphology |
| Infectious disease screening | Brucella canis, STIs | Negative results |
| Serial ultrasound | Ovarian and uterine structure | Normal ovarian activity, uterine lining |
| Body condition score | Weight relative to ideal | 4 to 5 on 9-point scale |
What you need to have on file
A thyroid screening conversation guide for your veterinarian
You are not the one creating a testing protocol. That is your veterinarian’s role. But you can prepare for an informed conversation. When you sit down with your vet to discuss thyroid screening for your breeding animals, here is what you should have in mind and be ready to discuss.
Know which five tests make up a complete thyroid panel and why each matters. Understand why testing should only be done when the dog is healthy and off medications. Be clear about when to start screening (around 1 year) and how often to retest. Ask your veterinarian which approved endocrinology laboratory they recommend. Discuss whether your breed has known baseline differences in thyroid values. Bring your records, previous test results, cycle data, and any observations that might help your veterinarian interpret the results in context.
The Orthopedic Foundation for Animals (OFA) and the Canine Health Information Center (CHIC) maintain databases where you can log results and track them over time. These registries also help you search pedigrees and research health trends within your breed.
| What to Discuss with Your Vet | Why It Matters | Your Role |
|---|---|---|
| The five tests in a complete panel | Ensures nothing is missed | Ask for these by name |
| Approved laboratory selection | Quality control standards differ | Use the lab your vet recommends |
| Washout period after illness/meds | Prevents false positives | Share medication history honestly |
| Breed-specific baseline values | Some breeds run naturally lower | Know your breed’s norms |
| OFA/CHIC registration | Tracks trends across generations | Log results after each test |
| Previous test results and cycle data | Context improves interpretation | Bring records to the appointment |
Body condition and breeding wellness scoring
Post a 9-point Body Condition Score chart where you can see it daily. Dogs in ideal breeding condition score 4 to 5 out of 9. Obesity and poor body condition both reduce fertility. You do not need complex tools to track this. A simple five-point Breeding Wellness Scorecard logs heat cycle regularity, recovery time after whelping, milk production quality, emotional engagement with litter, and litter size trends.
Review this scorecard before attributing fertility problems to the thyroid. Sometimes the answer is simpler: the dog is too heavy, recovering too slowly, or not eating adequately. Physical condition is the first place to look. It is also the most controllable variable you have.
| Wellness Factor | 1-2 (Poor) | 4-5 (Ideal) | 8-9 (Excessive) |
|---|---|---|---|
| Heat cycle regularity | Irregular, skipped cycles | Regular 18 to 24 day cycles | Hyperestrous or prolonged |
| Post-whelping recovery | >6 weeks to return to baseline | 2 to 4 weeks return | Severe depletion persists |
| Milk production | Insufficient for litter | Adequate, pups gain weight | Excessive, litter overfed |
| Maternal engagement | Neglectful, poor attentiveness | Responsive, engaged caregiving | Over-anxious, hovering |
| Litter size trend | Declining, ❤ pups | Consistent, 5 to 8 pups | Artificially inflated expectations |
The real question: should a hypothyroid dog be bred at all?
If your veterinarian confirms true hypothyroidism, the conversation should not jump straight to treatment and supplementation. The more important question is this: should this dog be part of your breeding program at all?
The rule of thumb in responsible breeding is simple: only breed healthy animals. Hypothyroidism, particularly autoimmune thyroiditis, has a genetic component. Breeding an affected animal means propagating the predisposition to future generations. You may fix the current dog’s symptoms with levothyroxine, but you do not fix the genetics. The offspring carry the risk forward.
This is a conversation to have with your veterinarian, not a decision to make alone. Consider the severity of the disease, the dog’s overall genetic contribution to your program, and whether the benefits of breeding that individual truly outweigh the risk of passing on a heritable condition. In most cases, the responsible decision is to remove the dog from the breeding program and focus your genetic investment on healthier individuals.
| Scenario | Breeding Decision | Rationale |
|---|---|---|
| Confirmed hypothyroidism (clinical signs + abnormal panel) | Remove from breeding program | Heritable condition; propagates risk to offspring |
| TgAA positive, all other tests normal | Keep in program, retest annually | No clinical disease yet; monitor for progression |
| TgAA positive, fT4 low, TSH high | Discuss removal with your veterinarian | Genetic risk is present and measurable |
| Multiple markers abnormal, clinical signs present | Remove from breeding program | Active disease; breeding would be irresponsible |
| Euthyroid sick (low T4 due to illness) | Continue breeding once recovered | Thyroid is healthy; illness was the cause |
What you need to watch for
Testing during illness or while on medications
This is the red flag that most often leads to false diagnosis. Non-thyroidal illnesses depress circulating T4. Sulfonamide antibiotics, glucocorticoid steroids, and phenobarbital all interfere with thyroid hormone metabolism. A dog recovering from infection, taking anti-inflammatory steroids, or being managed on seizure medication will show a falsely low T4. Testing at this moment creates a false positive and sets the path toward unnecessary supplementation.
Watch for the urge to test quickly when a dog is ill or recently completed a course of medications. Resist it. Work with your veterinarian to establish a washout period. Wait until the dog is fully recovered and all medications are cleared from the system. This discipline prevents false diagnoses and the cascade of consequences that follow.
| Condition / Medication | Effect on T4 | Washout Time | Test Result |
|---|---|---|---|
| Recent infection/fever | Temporarily lowered | 2 to 4 weeks recovery | False low T4 |
| Glucocorticoid therapy | Suppresses T4 during use | 2 to 4 weeks after stopping | False low T4 |
| Sulfonamide antibiotics | Lowers T4 while on drug | 1 to 2 weeks after stopping | False low T4 |
| Phenobarbital (seizure mgmt) | Increases metabolism | 4 to 8 weeks after stopping | May appear low |
| Illness resolved | Returns to baseline | Once fully recovered | Normalizes |
TgAA-positive, euthyroid dogs: do not remove them prematurely
A positive thyroglobulin autoantibody result triggers panic. “The immune system is attacking my dog’s thyroid.” The instinct is to remove the dog from the breeding program immediately. Stop. If the dog’s other thyroid function tests are normal, the dog is euthyroid. Having thyroglobulin autoantibodies does not mean clinical hypothyroidism has developed.
What it means is that this dog has a higher risk of developing hypothyroidism over time. The correct action is to keep the dog in the program but retest annually. Monitor for signs of progression. Do not throw away genetic diversity for other valuable traits just because of a positive autoantibody. Many excellent breeding animals carry TgAA without ever showing clinical disease. Your role is to watch them, not to remove them prematurely from the program.
| TgAA Result | Other Tests | Action | Retest Interval |
|---|---|---|---|
| Negative | All normal | Continue breeding | Every 1 to 2 years |
| Positive | fT4, TSH, T4 all normal | Keep in program, monitor closely | Annually |
| Positive | fT4 low, TSH high | Genetic risk present, discuss with vet | Every 6 to 12 months |
| Positive | Multiple markers abnormal | Clinical disease developing, consider removal | Monitor closely |
Slow-onset systemic signs indicating disease progression
Hypothyroidism progresses slowly. Months or even years may pass before obvious clinical signs appear. Watch for unexplained weight gain despite consistent feeding. Notice lethargy or mental dullness where the dog used to be alert. Look for hair coat changes: alopecia (hair loss), seborrhea (flaky, oily skin), or a dull, brittle coat. These are often subtle at first. You notice them because you handle the dog daily and know its normal appearance. Your veterinarian may not see these signs in a brief exam.
Trust your observations. If a dog positive for thyroglobulin autoantibodies begins showing these systemic signs, increase monitoring frequency. Retest the thyroid panel. Report findings to your veterinarian. Remember: when hypothyroidism causes infertility, these other signs are almost always present too. They are the warning system. Pay attention to them.
| Early Sign | Timeline | Next Step | Significance |
|---|---|---|---|
| Unexplained weight gain | Weeks to months | Monitor diet, exercise, check BCS | Possible early metabolic shift |
| Lethargy, dull mentation | Weeks to months | Note frequency and severity | Behavioral change may precede labs |
| Hair loss (alopecia) | Weeks to months | Document location and extent | Common early dermatologic sign |
| Seborrhea, poor coat | Months | Photograph for vet reference | Skin barrier dysfunction |
| Cold intolerance | Months to years | Note seasonal patterns | Late-stage sign of progression |
| Reproductive issues appear | Variable | Retest thyroid immediately | May be linked if systemic signs present |
Conclusion
Hypothyroidism in breeding dogs is real, but it is not the common cause of infertility that many believe it to be. When hypothyroidism does affect fertility, other clinical signs are almost always present: weight gain, lethargy, coat changes. If your dog has none of these symptoms, the thyroid is very unlikely to be the culprit. Look elsewhere first.
Overdiagnosis is also real, and it leads to unnecessary medication, masked underlying causes of reproductive failure, and unjustified loss of valuable genetic material. Your job is not to diagnose, that is your veterinarian’s role, but to observe, document, and demand rigorous evidence before accepting a diagnosis. A single T4 test is not rigorous. A complete thyroid panel from an approved laboratory, performed on a healthy dog, with full rule-out of other causes is.
Screening begins at age 1 and continues every 1 to 2 years while the dog breeds. You keep records, track trends, and watch for systemic signs that suggest disease progression. You do not panic at a positive thyroglobulin autoantibody if other markers are normal. You resist the urge to supplement without evidence. And if a dog is confirmed hypothyroid, you ask the harder question: should this animal be bred at all? Only healthy animals belong in a breeding program. That is how you protect the next generation.
A test is only as good as its interpretation. This is the science-first, evidence-based approach. It honors both your experience as a breeder and the expertise of your veterinarian. Together, you build a program that lasts.
Want to put all of this into action during your next health screening? Inside the Breeder Vault, you’ll find the Hypothyroidism Screening Field Protocol, a printable decision tree with test interpretation guides, veterinary request scripts, and emergency thresholds designed to be used in real time. It is the operational companion to everything you just learned.