🇫🇷 Lire en Français | 🇪🇸Leer en Español | 🇧🇷Leia em português
The queen labors through the night. By dawn, a healthy litter sprawls across the whelping box: five kittens, all moving, all warm. You breathe. But as you watch, one kitten circles the dam’s rear, searching, failing to latch. The clock has already started ticking. Colostrum flows for fewer than 24 hours from the moment the first kitten arrives. After that, the dam’s milk remains nourishing, but it will never again carry the concentrated antibody payload that shields a newborn from bacterial, viral, and parasitic threats. If this kitten does not nurse in the next 12 hours, the window closes. Permanently.
This is not theory. As a veterinarian, I have watched litters thrive and collapse in the space of a week, often because a single critical moment was missed or misunderstood. Colostrum is your single greatest tool for launching immunity in the neonatal period. When it works, kittens enter the world with a one-time security download of maternal protection. When it fails, even by a few hours, the consequences compound across the first 6 to 8 weeks of life.
This post transforms what many breeders know intuitively into actionable protocols: exactly what to look for, how much is enough, what to do when it isn’t, and how to monitor immunity in the vulnerable neonatal period. You will learn the precise timeline of immunoglobulin transfer, how to recognize colostrum failure before it’s too late, and when serum supplementation or other rescue measures are appropriate.
- TL;DR: What You Need to Know
- What You Need to Know: The Immunology of Colostrum Transfer
- What You Need to Do: Maximizing Colostrum Transfer in the First Hours
- What You Need to Have Ready: Rescue Protocols When Colostrum Fails
- What You Need to Watch For: Monitoring Immunity in the Vulnerable Neonatal Period
- Conclusion: Prevention, Recognition, and Action
TL;DR: What You Need to Know
- Kitten colostrum immunity transfer occurs almost exclusively in the first 12 to 16 hours after birth; the absorption window closes by 24 hours.
- Feline colostrum IgG concentration drops 5-fold over the first 7 days of lactation, making early nursing the most critical protective window.
- A kitten colostrum immunity goal is 22 mL/kg (0.33 fl oz/lb) of colostrum ingested within the first few hours after birth.
- Colostrum failure is recognizable through dam-side indicators (weak letdown, low volume, visible signs of illness) and kitten-side indicators (refusal to nurse, weak suck, weight loss despite apparent nursing).
- Serum supplementation and supportive feeding protocols exist for colostrum-deprived kittens, but are most effective when begun immediately after colostrum failure is recognized.
- Colostrum-deprived kittens remain vulnerable to infection until primary vaccination series is complete; the immunity gap extends roughly 6 to 8 weeks after birth.
- Neonatal erythrolysis (blood type incompatibility) can make colostrum unsafe in some multi-cat matings; type-A kittens nursing type-B dams are at highest risk.
What You Need to Know: The Immunology of Colostrum Transfer
What Colostrum Delivers in the First Nursing Session
Colostrum is the first immune gift your kitten will ever receive. In the first 24 hours after queening, the dam produces a thick, yellowish fluid loaded with immunoglobulins, particularly IgG and IgA. These antibodies represent a snapshot of threats the queen has encountered or is vaccinated for: feline panleukopenia virus, feline herpesvirus, feline calicivirus, common bacterial pathogens. They transfer directly to the nursing kitten, providing immediate passive immune protection.
Think of it as a one-time security download. The queen has built immunity over her lifetime. She passes that entire defense library to her kittens in condensed form, all within the first 24 hours. Mature milk, which appears after 3 to 4 days of lactation, contains far lower concentrations of immunoglobulins. The composition shift is dramatic and biological.
| Component | Colostrum (Hours 0–12) | Mature Milk (Days 3–7) | Function |
|---|---|---|---|
| IgG (mg/mL) | 50–100 | 5–10 | Primary passive immunity; opsonizes pathogens |
| IgA (mg/mL) | 5–15 | 1–3 | Mucosal immunity; protects intestinal and respiratory epithelium |
| Protein (g/100 mL) | 15–20 | 6–8 | Total protein; supports neonatal metabolism |
| Fat (g/100 mL) | 4–6 | 4–5 | Caloric density; stable between colostrum and mature milk |
| Lactoferrin (mg/mL) | 0.5–1.5 | 0.1–0.3 | Antimicrobial; iron-binding capacity |
| White blood cells (cells/mL) | 500–2000 | 50–200 | Lymphocytes, macrophages; more abundant in colostrum |
The Absorption Window: A Door That Only Opens Once
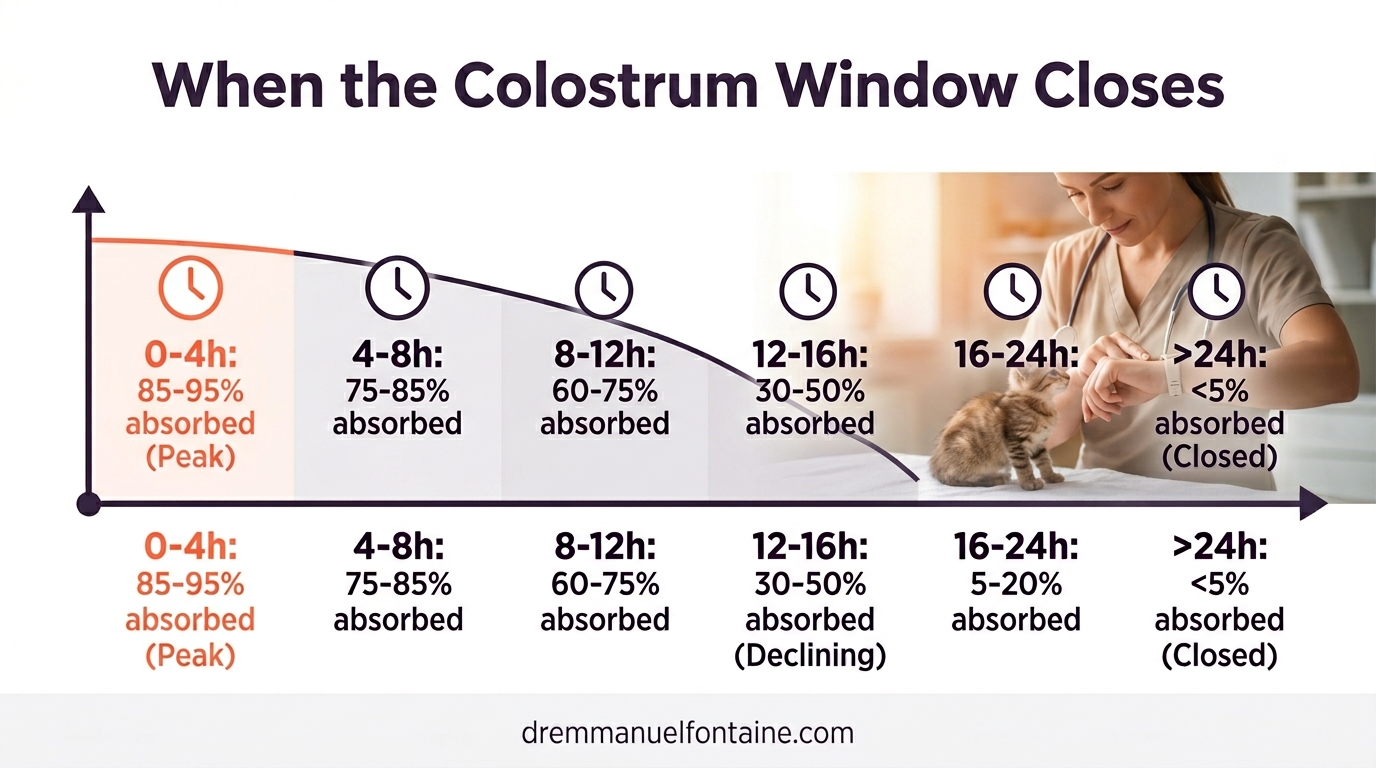
A kitten’s intestinal epithelium is initially permeable to large proteins, including intact immunoglobulin molecules. This is not a design flaw. It is a feature. The permeable state is temporary by evolutionary design. Beginning around 12 hours of age and largely complete by 24 hours, the intestinal barrier closes, becoming impermeable to macromolecules. Think of it as a gate. The gate is open for exactly one reason: to let the largest, most critical immune molecules cross. Once it closes, nothing that large gets through again.
After intestinal closure, antibodies in milk are still present. The kitten still has the milk. But the antibodies cannot be absorbed. They remain in the intestinal lumen and are eventually eliminated in feces. A kitten that does not nurse colostrum in the first 12 to 16 hours will not absorb significant immunoglobulin regardless of how much milk is offered later.
| Age (Hours) | Absorption Efficiency (%) | Cumulative IgG Absorbed (mL equivalent) | Practical Implication |
|---|---|---|---|
| 0–4 | 85–95 | High (first doses most critical) | Peak absorption; most critical hours |
| 4–8 | 75–85 | Continued strong absorption | Still highly effective |
| 8–12 | 60–75 | Moderate absorption; decline begins | Absorption declining but still functional |
| 12–16 | 30–50 | Weak absorption | Kitten likely missing significant immunity |
| 16–24 | 5–20 | Negligible absorption | Intestinal closure imminent or complete |
| >24 | <5 | Minimal; immune passive transfer incomplete | Window effectively closed; active immunity not yet established |
Why Feline IgG Concentration Falls Sharply in Early Lactation
One of the most dangerous assumptions a breeder can make is that if a kitten misses the first 24 hours, it can catch up by nursing freely in days 2 to 7. This assumption is wrong. The queen’s colostrum is most protective on day 1 because her IgG concentration is highest. As lactation matures, IgG concentration falls sharply. By day 7, colostrum-stage milk contains one-fifth the immunoglobulin it did on day 1.
This is not avoidable. The queen’s body is transitioning from colostrum production to milk production, and this transition prioritizes nutritional content (fat, lactose, casein) over immune factors. The mechanics are clear: as milk composition changes to optimize growth, immune factors are diluted. A kitten born into a litter where nursing was delayed cannot make up for missed colostrum by nursing more from days 2 to 7. The immunoglobulin simply is not there in the same concentration.
| Day of Lactation | IgG Concentration (mg/mL) | % of Day 1 Concentration | Relative Protective Value |
|---|---|---|---|
| 1 | 80 | 100% | Peak protection; colostrum stage |
| 2 | 50 | 63% | High protection; transitional milk |
| 3 | 30 | 38% | Moderate protection; maturing milk |
| 4 | 18 | 23% | Declining protection; mature milk |
| 5 | 12 | 15% | Low protection; established mature milk |
| 6–7 | 16 | 20% | Low and stable; mature milk plateau |
What You Need to Do: Maximizing Colostrum Transfer in the First Hours
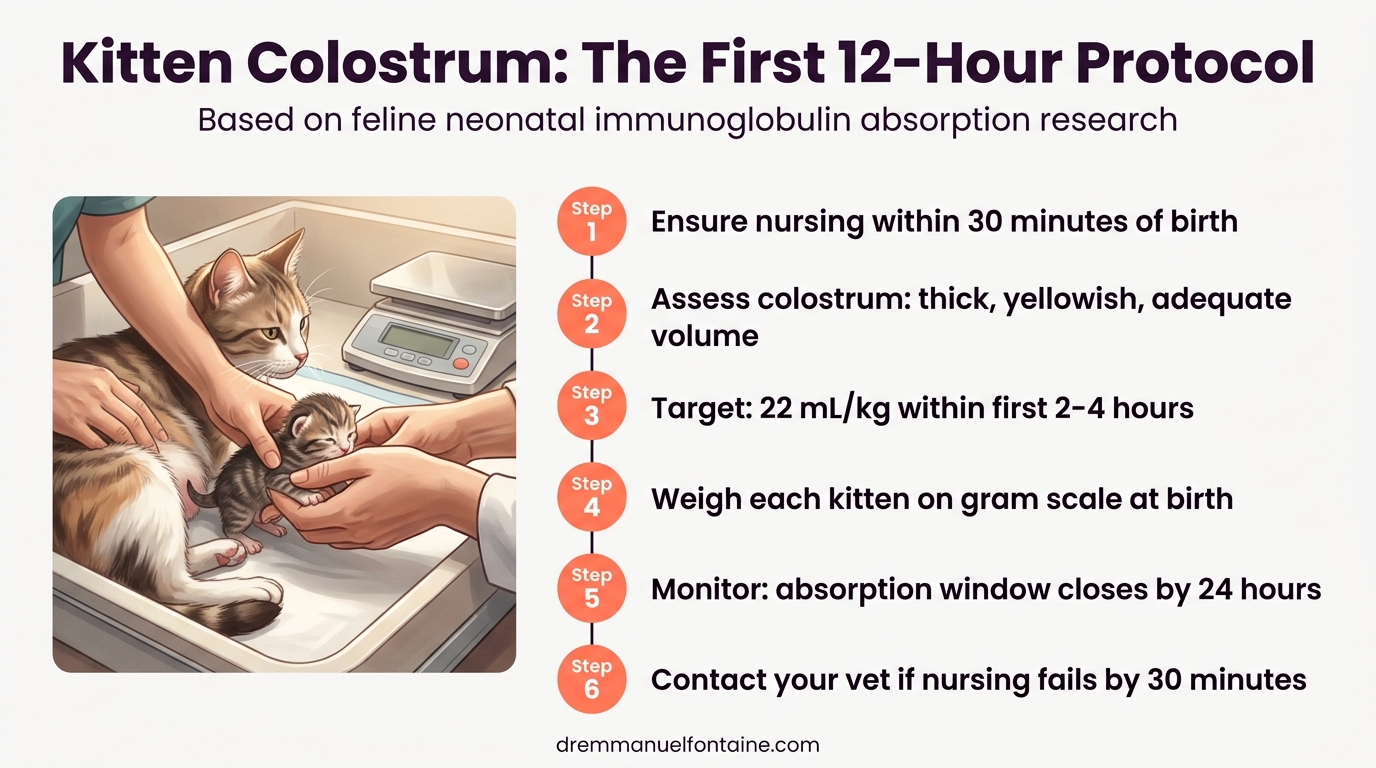
Getting Kittens Nursing Within 30 Minutes of Birth
Prevention is the strongest strategy. A breeder cannot guarantee perfect colostrum transfer, but can eliminate preventable delays. Newborn kittens are naturally motivated to nurse within 15 to 30 minutes of birth if the queen is healthy, alert, and able to position herself for nursing. The dam’s letdown reflex (milk ejection) is strongest immediately after birth, driven by oxytocin released during labor and the tactile stimulus of kittens suckling.
If a kitten is not nursing by 30 minutes of age, assess the dam’s condition and kitten responsiveness. Weak kittens, exhausted dams, or abnormal presentations can delay nursing. Your veterinarian should be consulted if a kitten is not nursing or if the dam is not allowing nursing. The checklist below outlines the critical first-hour protocol to maximize colostrum transfer from the start.
| Time Window | Action | Success Indicator | If Not Achieved, Next Step |
|---|---|---|---|
| 0–10 min | Kitten dries; dam cleans kitten | Kitten is warm, responsive | Assist drying if needed; monitor warmth |
| 10–15 min | Position kitten at teat; observe latch | Kitten latches and begins suckling | Gently reposition; ensure teat accessibility |
| 15–30 min | Confirm active nursing of colostrum-stage milk | Kitten is suckling audibly; dam is comfortable | If not nursing: assess kitten alertness and dam letdown |
| 30–60 min | All kittens in litter should have nursed once | Each kitten has accessed colostrum | If any kitten has not: hand-feeding of expressed colostrum |
| 60–120 min | Confirm second nursing bout begins | Kittens returning to dam for additional feeds | Interval between bouts should narrow as dam settles |
| 2–6 hours | Monitor continued nursing pattern | Kittens nursing every 30–90 minutes | Contact vet if nursing stops or becomes infrequent |
Assessing Colostrum Quality and Quantity at the Queen Level
Not all colostrum is created equal. The queen’s health, nutrition, immune history, and vaccination status all influence colostrum composition. Additionally, some queens produce abundant colostrum while others produce minimal amounts despite being healthy. A breeder who can assess colostrum visually and through observation of the dam can catch problems early.
Colostrum appears as a thick, yellowish fluid; mature milk is whiter and thinner. If colostrum appears watery, discolored, or is scant in volume, the dam may be ill, nutritionally depleted, or have a systemic condition affecting lactation.
| Assessment | Normal / Adequate | Red Flag / Inadequate | Action |
|---|---|---|---|
| Color | Yellowish, opaque | Clear, watery, or stained (brown/red) | Consult vet; consider colostrum supplementation |
| Consistency | Thick, creamy; clings to teat | Watery, drips freely | Likely low immunoglobulin; supplement |
| Quantity (subjective) | Visible droplets at each teat; dam drips | No visible milk; dam must be stimulated | Likely insufficient volume; plan supplementation |
| Dam behavior | Alert, nesting; accepts kittens; responsive letdown | Lethargic, febrile, rejecting kittens, painful | Do not rely on colostrum; seek vet care immediately |
| Timing of appearance | Within 2–4 hours of first kitten birth | Delayed beyond 6 hours; no visible colostrum | Contact vet; may indicate systemic issue |
| Odor | Slightly sweet; no foul smell | Foul, acrid, or fetid odor | Potential infection; colostrum should not be used |
Volume Targets: The 22 mL/kg Benchmark
A kitten must ingest sufficient colostrum volume to receive a meaningful dose of immunoglobulin. Research in feline neonatology suggests that a kitten ingesting 22 mL/kg (0.33 fl oz/lb) of colostrum achieves adequate passive immunity transfer. This is a practical target. If a kitten weighs 100 grams at birth, the goal is 2.2 mL (0.07 fl oz) of colostrum ingested. A 150-gram kitten needs 3.3 mL (0.11 fl oz).
Most healthy kittens nursing freely from an adequate dam achieve this volume within the first 2 to 4 hours of life without intervention. However, if a kitten is nursing weakly, if the dam is producing scant colostrum, or if a kitten is separated from the dam, the breeder must ensure the kitten receives at least this volume through hand-feeding.
| Kitten Birth Weight | Recommended Colostrum Volume (mL) | Recommended Colostrum Volume (fl oz) | Typical Delivery Method |
|---|---|---|---|
| 80–100 g | 1.8–2.2 mL | 0.06–0.07 fl oz | Bottle or syringe; 3–4 small feeds |
| 100–120 g | 2.2–2.6 mL | 0.07–0.09 fl oz | Bottle or syringe; 3–4 feeds |
| 120–150 g | 2.6–3.3 mL | 0.09–0.11 fl oz | Bottle or syringe; 3–4 feeds |
| 150–180 g | 3.3–4.0 mL | 0.11–0.13 fl oz | Bottle or syringe; 3–4 feeds |
| 180–200 g | 4.0–4.4 mL | 0.13–0.15 fl oz | Bottle or syringe; 4–5 feeds |
What You Need to Have Ready: Rescue Protocols When Colostrum Fails
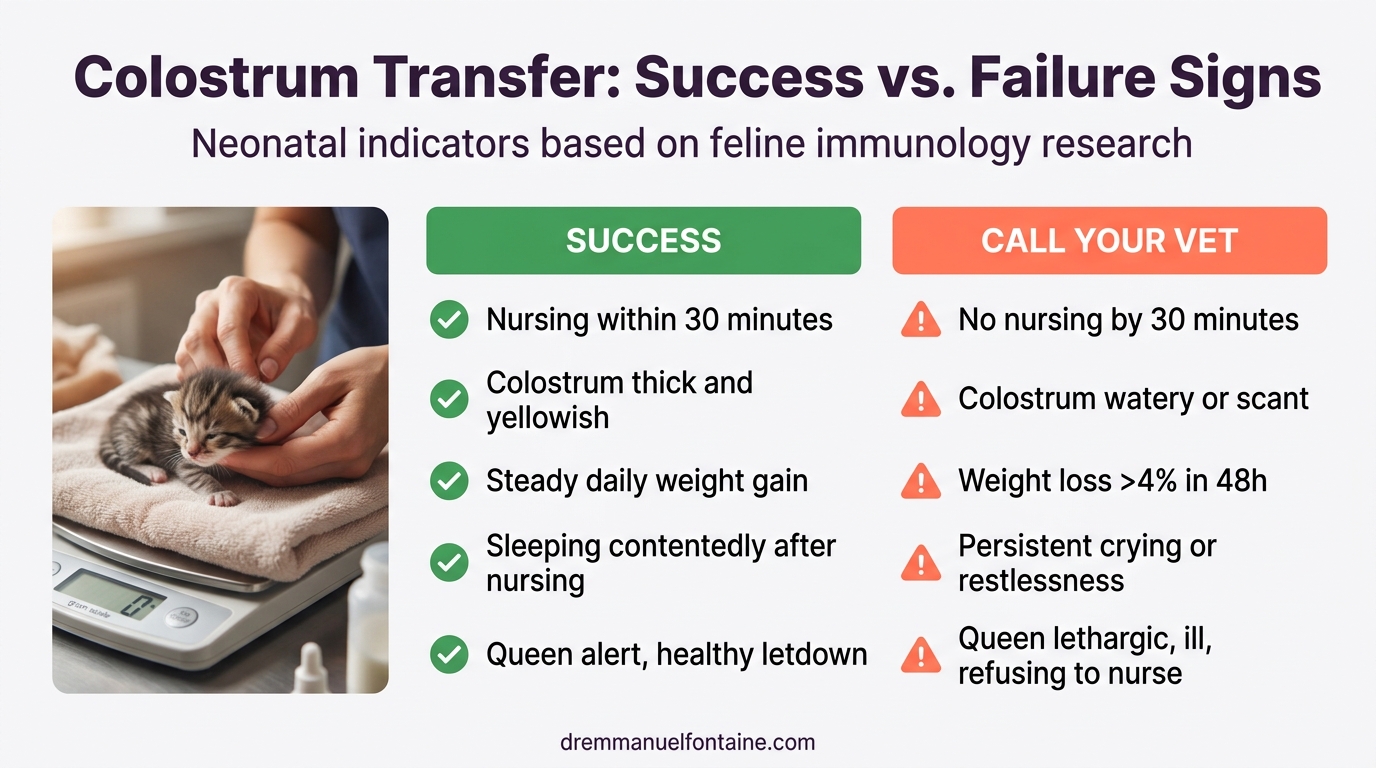
Recognizing Colostrum Failure Before It’s Too Late
Colostrum failure is not always obvious. Some kittens may appear to be nursing normally but are actually receiving minimal immunoglobulin due to inadequate dam output or absorption problems. Other colostrum failures are acute: the dam becomes ill, a kitten is orphaned, or a kitten is too weak to nurse. A breeder who recognizes the signs of failed colostrum transfer can intervene within the critical 12 to 24 hour window when alternative interventions remain effective.
The signs of successful colostrum transfer include kittens that nurse vigorously, gain weight consistently, sleep contentedly, and show no signs of dehydration. The signs of failed colostrum transfer include weak nursing, refusal to latch, persistent crying, weight loss despite apparent nursing, and (after 24 to 48 hours) early infection signs like lethargy or fever. Work with your veterinarian to establish a monitoring protocol: daily weights, observation of nursing behavior, and prompt action if the pattern breaks.
| Sign | Successful Colostrum Transfer | Failed Colostrum Transfer | Timeline |
|---|---|---|---|
| Nursing vigor | Strong latch; audible swallowing; dam comfortable | Weak suck; kitten struggles to latch; repeated failed attempts | First 2–4 hours |
| Weight change (birth + 24 h) | Gain | Loss or plateau; no recovery attempt by 24 hours | First 24 hours |
| Kitten alertness | Alert between feeds; eyes open; responsive | Lethargic, weak cry, slow to respond | Hours 4–24 |
| Stool passage | Meconium passed by 24 h; may see transitional stools by 48 h | No stool passage by 24 h; or diarrhea (suggests enteric challenge) | First 24–48 hours |
| Early infection signs | None; kitten is warm, normal temperature | Fever (>39.5°C / 103°F), lethargy, reluctance to nurse | Hours 24–48 |
Serum Supplementation: When and How to Use It
When colostrum-deprived kittens are identified within 24 to 36 hours of birth, serum supplementation is a viable rescue protocol. Serum contains antibodies and is absorbed more efficiently by the kitten after intestinal closure than colostrum would be (though not as efficiently as colostrum itself during the open window). Ideally, serum comes from the dam (if available and healthy) or from an adult cat in the same household with known exposure to common feline pathogens.
Serum is administered intravenously (IV) for maximum absorption. Subcutaneous (SQ) or intraperitoneal (IP) administration is less efficient but may be used if IV access is not feasible. A single dose typically provides 12 to 48 hours of additional antibody coverage while the kitten’s own immune system mounts primary responses to vaccination. Consult your veterinarian for serum sourcing and administration.
Feline Milk Replacer and Supportive Care for Deprived Kittens
A colostrum-deprived kitten must receive adequate nutrition and supportive care while passive immunity protection is limited. Feline milk replacer (formulated for kittens, not humans) provides the protein, fat, and caloric density needed for growth. While milk replacer does not replace colostrum’s immune function, it supports the kitten’s metabolic and growth demands so that when active immunity (from vaccination) begins, the kitten has reserves to mount a strong response.
Supportive care also includes environmental warmth, hygiene, and monitoring for early infection. A colostrum-deprived kitten is at elevated risk for bacterial and viral infections for the first 6 to 8 weeks of life, until the primary vaccination series is complete and active immunity is established.
| Age & Colostrum Status | Primary Nutrition | Feeding Frequency | Infection Monitoring | Veterinary Contact |
|---|---|---|---|---|
| 0–7 days; colostrum received | Dam nursing (primary); no supplement needed | Ad lib; typically 8–12 bouts/day | Daily weight checks; stool observation | Routine postpartum check |
| 0–7 days; colostrum failed | Feline milk replacer + supportive dam nursing if possible | Every 2–3 hours; 8–10 feeds/day | Daily weight; temperature checks twice daily | Immediate vet consult; likely daily check-ins |
| 7–14 days; adequate colostrum history | Dam nursing; begin introducing wet kitten food at day 10 | Gradually transition to 4–5 meals/day | Weekly weight checks; stool quality | Routine weaning-phase monitoring |
| 7–14 days; colostrum failure | High-quality feline milk replacer; continue supportive dam nursing | Every 3–4 hours; 5–7 feeds/day | Every 1–2 days temperature; alert for lethargy, diarrhea | Veterinary check every 3–5 days until 14 days old |
| 2–4 weeks; past neonatal stage | Wet kitten food (primary); milk replacer supplement | 3–4 meals/day | Weekly weight; continue infection surveillance | Advance vaccination schedule if colostrum failed |
What You Need to Watch For: Monitoring Immunity in the Vulnerable Neonatal Period
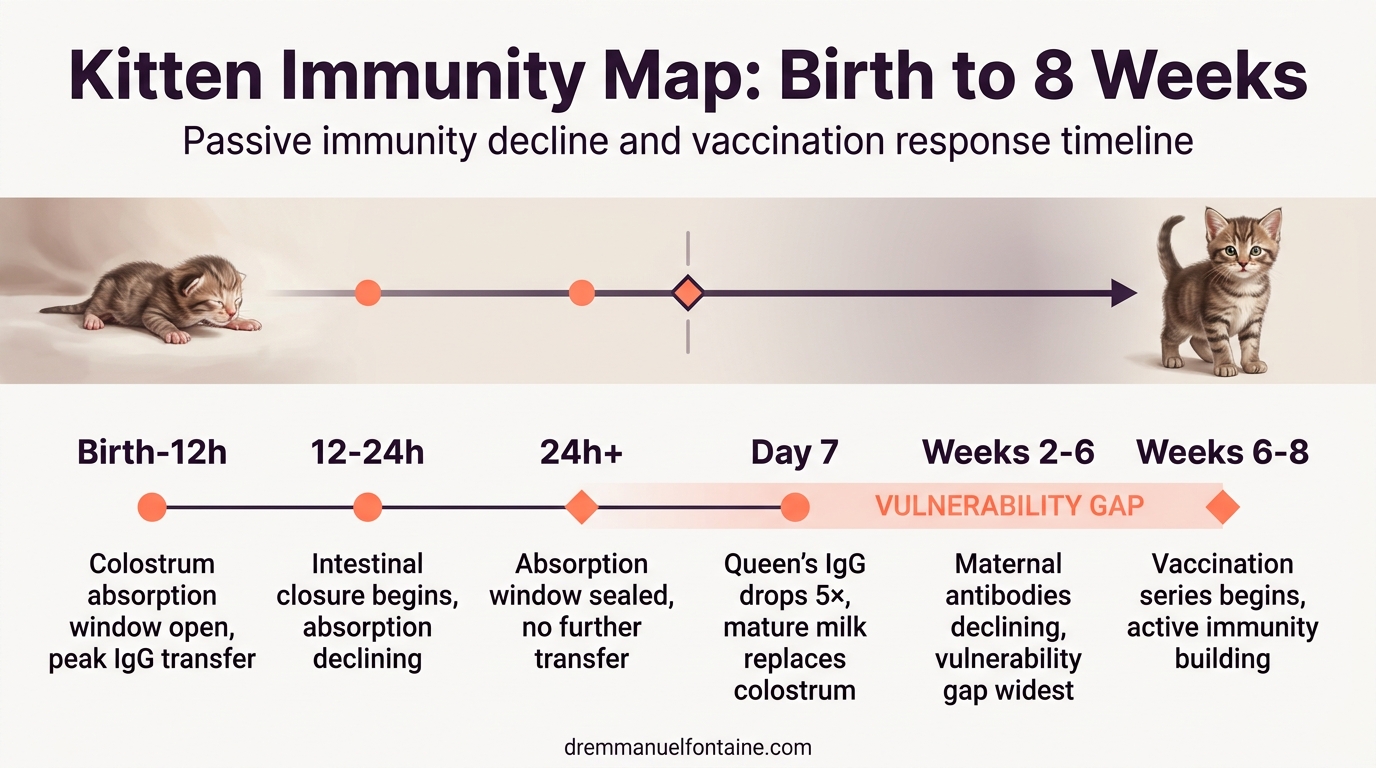
The Immunity Gap Between Colostral Protection and Vaccination
A kitten born to a vaccinated dam with adequate colostrum receives passive immunity that declines over 6 to 8 weeks as maternal antibodies are metabolized. Simultaneously, the kitten’s own immune system must be trained through vaccination to recognize and respond to threats. During the transition, roughly weeks 2 to 8, the kitten is partially protected by declining maternal antibodies while primary vaccination responses are developing. If colostrum transfer fails, this gap widens and the kitten is left vulnerable with minimal passive protection and no active immunity yet in place.
Standard feline vaccination begins at 6 to 8 weeks of age with a series of doses 3 to 4 weeks apart. A kitten with adequate colostrum history tolerates this timeline well. A colostrum-deprived kitten may benefit from earlier vaccination (as early as 4 weeks) and closer follow-up, depending on infection risk and veterinary assessment. Your veterinarian can advise on customizing the vaccination timeline to account for colostrum status.
| Age (Weeks) | Maternal Antibody Level | Vaccination Response Quality | Vulnerability Gap | Practical Implication |
|---|---|---|---|---|
| 0–1 | Maximum (from colostrum) | No active response yet | Minimal; colostrum is primary defense | Protect from environmental exposure; ensure nursing |
| 2–3 | High (80–100% of initial) | Initial response begins | Minimal; maternal antibodies still dominant | Continue standard vaccination prep |
| 3–4 | Moderate-high (60–80%) | Response building; interference may occur | Moderate; maternal antibodies may suppress response | Time first vaccine carefully (work with vet) |
| 4–6 | Moderate (40–60%) | Active immunity developing; less maternal interference | Moderate-high; protection is mixed | If colostrum-deprived, consider vaccination at 4 weeks |
| 6–8 | Low-moderate (20–40%) | Strong active response by week 8 | Moderate; still transitioning | Standard first vaccination window; booster at 3–4 weeks |
| 8–12 | Minimal (<20%) | Peak active immunity response post-booster | Minimal by week 12; active immunity established | Booster vaccination complete; active immunity now primary |
Infection Patterns in Colostrum-Deprived Kittens
Colostrum-deprived kittens show distinct infection vulnerability patterns. They are at elevated risk for bacterial infections (Escherichia coli, Staphylococcus species) in the first 1 to 2 weeks of life, and for viral infections (feline panleukopenia, feline herpesvirus, feline calicivirus) from weeks 2 to 6 onward. Early bacterial infections are often triggered by environmental exposure or minor trauma (umbilical cord issues, skin breakdown), while viral infections are usually acquired through the environment or dam shedding.
Recognizing these patterns allows a breeder to monitor more carefully and consult a veterinarian promptly if warning signs appear. A single episode of diarrhea in a well-colostred kitten may resolve on its own; the same sign in a colostrum-deprived kitten warrants immediate investigation. Work with your veterinarian to establish an infection surveillance protocol appropriate to your kitten’s risk profile.
| Age | Primary Infection Risk | Early Warning Sign | Moderate Warning Sign | Urgent Sign (Call Vet Immediately) |
|---|---|---|---|---|
| 0–7 days | Bacterial (umbilical, skin) | Lethargy; reduced nursing | Fever (>39.5°C / 103°F); diarrhea | Severe lethargy; refusal to nurse; abdominal distension |
| 7–14 days | Bacterial, viral (early) | Mild lethargy; inconsistent appetite | Fever; diarrhea; sneezing or nasal discharge | High fever (>40°C / 104°F); dehydration; respiratory distress |
| 2–4 weeks | Viral (panleukopenia, herpesvirus, calicivirus) | Sneezing; mild ocular discharge | Fever; diarrhea; vomiting; oral ulcers or conjunctivitis | High fever; severe diarrhea; reluctance to eat; neurological signs |
| 4–8 weeks | Viral (persistent or secondary) | Mild respiratory symptoms; occasional coughing | Persistent fever; diarrhea; ocular discharge | Respiratory distress; severe dehydration; failure to gain weight |
When Neonatal Erythrolysis Prevents Colostrum Use
Neonatal erythrolysis is a serious condition in which a kitten is born to a dam with incompatible blood type. The dam’s colostrum contains high-titer antibodies against the kitten’s blood type (naturally occurring, not from prior transfusion). When the kitten ingests this colostrum, the antibodies attack and destroy the kitten’s red blood cells, causing hemolytic anemia, jaundice, and potentially death. In domestic cats, the primary risk is a type-A kitten born to a type-B dam.
Prevention requires knowing dam and sire blood types before breeding. A type-B dam should never be bred to a type-A sire if neonatal erythrolysis is a concern in the breeding program. If a type-B dam is bred to a type-A or AB sire and kittens of unknown type are born, blood typing is recommended before allowing colostrum nursing. Some breeders choose to hand-feed colostrum-deprived kittens from type-B dams rather than risk erythrolysis. Your veterinarian can advise on blood typing and safe colostrum protocols if type incompatibility is a risk in your pedigree.
| Dam Blood Type | Kitten Blood Type | Colostrum Safe? | Risk Level | Recommended Protocol |
|---|---|---|---|---|
| Type A | Type A | Yes | None | Normal colostrum nursing |
| Type A | Type B | Yes | None | Normal colostrum nursing |
| Type A | Type AB | Yes | None | Normal colostrum nursing |
| Type B | Type A | No | Very High (erythrolysis likely) | Hand-feed colostrum from typed donor or supplement with serum |
| Type B | Type B | Yes | None | Normal colostrum nursing |
| Type B | Type AB | Yes | None | Normal colostrum nursing |
Decision Framework for Colostrum Supplementation (NEW)
When faced with a potential colostrum failure, use this framework to determine whether immediate hand-feeding, serum supplementation, or close monitoring is most appropriate. The key variables are timing (how many hours post-birth), kitten vigor, and dam colostrum quality.
An orphaned litter or a kitten with absorption problems may benefit from emergency hand-feeding protocols to bridge the neonatal period safely. The following decision table guides immediate intervention choices.
| Hours Since Birth | Dam Colostrum Status | Kitten Nursing Vigor | Recommended Action | Timeline for Result |
|---|---|---|---|---|
| 0–4 | Adequate | Strong | Monitor closely; no intervention yet | Assess at 12 hours |
| 0–4 | Inadequate or absent | Any | Begin hand-feeding colostrum or substitute immediately | Supplement every 2 hours |
| 4–8 | Adequate | Weak but improving | Assist nursing; hand-feed supplement if intake is low | Recheck weight at 8 hours |
| 4–8 | Inadequate | Any | Hand-feeding mandatory; assess for serum at 12–24 hours if needed | Continue every 2–3 hours |
| 8–12 | Adequate | Strong and weight stable | Continue nursing; window still partially open | Final critical period |
| 12–24 | Any | Any weakness noted | Serum supplementation recommended if not already given | Begin IV/IP serum if available |
| 24+ | Any | Showed prior weakness | Supportive care only; serum unlikely to help; intensive monitoring | Vaccination at earliest opportunity |
Conclusion: Prevention, Recognition, and Action
Colostrum failure is not inevitable, and it is not a death sentence when it occurs. The difference between a lost litter and a healthy one often lies in early recognition and rapid intervention. You now understand the immunological window (12 to 24 hours), the warning signs that colostrum transfer is failing, and the rescue protocols available when it does. You know that passive immunity declines over weeks while active immunity develops, and that colostrum-deprived kittens require closer monitoring and possibly adjusted vaccination timelines.
The most important action is prevention: ensure nursing begins within 30 minutes of birth, assess colostrum quality and quantity in the first hours, and intervene immediately if a kitten is not nursing or the dam is not producing adequate colostrum. If colostrum failure is already happening, contact your veterinarian without delay. Serum supplementation, intensive supportive feeding, and close monitoring can salvage the outcome even after colostrum transfer has failed.
Your role as a breeder includes understanding this window, preparing for it, and executing these protocols calmly and swiftly when needed. A kitten that receives 22 mL/kg of quality colostrum in the first 12 hours enters the neonatal period with protection against the threats your herd encounters. A kitten that misses that window but receives serum supplementation and careful monitoring has a strong chance of thriving as active immunity develops. The path forward is knowledge, preparation, and action.
Want to put all of this into action with your next litter? Inside the Breeder Vault, you will find the Colostrum and Kittens’ Immunity Field Protocol, a printable monitoring checklist with decision trees, emergency thresholds, and veterinary request scripts designed to be used in real time. It is the operational companion to everything you just learned.