
🇫🇷 Lire en Français | 🇪🇸Leer en Español | 🇧🇷Leia em português
It is 2 a.m. You are on the floor beside the queening box. Your queen has been straining for what feels like an hour, but you cannot be sure because you stopped looking at the clock somewhere around midnight. A kitten was born fine at eleven-thirty. Nothing since. She is not distressed, not collapsed, not even panting, and that calm is what paralyzes you. Is she resting, or is she in trouble?
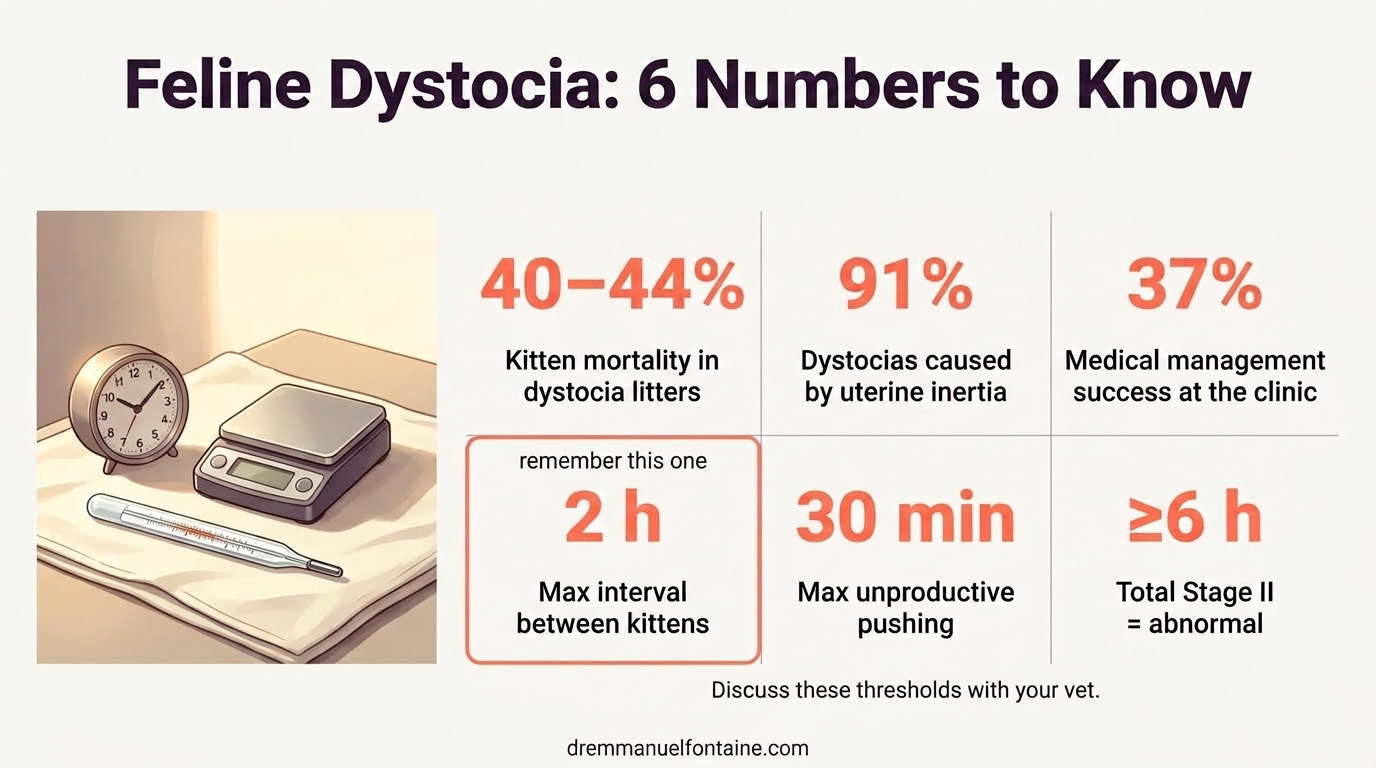
This is the moment dystocia takes lives. Not in the obvious emergency: the collapsed queen, the dark brown-black discharge, the kitten stuck in the canal. Those are easy calls. It takes lives in the quiet middle, when a stoic queen looks fine while her uterus has already stopped working. Feline dystocia runs a kitten mortality rate of roughly 40% to 44%, and the single biggest lever on that number is how fast you recognize it and reach your vet.
I wrote this as the breeder-facing companion to the clinical picture I share with veterinarians. Your job tonight is not to diagnose. Your job is to observe, time, and call. This post gives you the rules that make that call unambiguous, the biology behind the rules, and a preview of what your vet will assess when you arrive. The flowchart on your wall is the 2 a.m. first-responder tool. Your vet is still the one who saves the litter.
- The Biology Behind the Struggle
- The 2-Hour Rule and the 30-Minute Rule
- What You Keep Ready Before Labor Begins
- The Signs That Tell You the Next Minute Matters
- Conclusion
TL;DR
- Feline dystocia kills 40% to 44% of kittens in affected litters. Early recognition is the strongest lever you have.
- The two rules you never break: more than 30 minutes of strong, unproductive contractions or more than 2 hours between kittens means you are already on the phone to your vet.
- Uterine inertia causes up to 91% of feline dystocia cases. The uterus simply stops contracting, usually quietly.
- Breed risk is not just about flat faces. British Shorthair, Oriental breeds, Ragdoll, Birman and Abyssinian queens sit at the top of the insurance-database risk index. Domestic shorthairs sit at the very bottom.
- At the clinic, medical management with calcium and oxytocin succeeds in roughly 37% of feline dystocias. Surgery, not medication, saves most litters.
- Oxytocin is a veterinary drug, full stop. It is never administered at home. Your role is transport and timing; every drug decision belongs to your vet after an in-clinic assessment.
- Keep a printed red-flag list on the queening box wall. Your future 3 a.m. self needs bullets, not essays.
The Biology Behind the Struggle
Queens are stoic, but the labor clock is strict
Cats are quiet labor athletes. A queen in a well-set nesting box will often give you very little visible drama through the first stage of labor, the phase where the cervix dilates and she starts looking for her spot. That first stage can legitimately run 12 to 24 hours with no obvious contractions, only restlessness, quiet panting, or a refusal to eat. This is where breeders burn their observation budget guessing.
The rules tighten sharply once she enters stage II, active expulsion. A queen who is straining hard without producing a kitten is on a clock, and so is a queen in the rest interval between kittens. Two numbers anchor everything that follows: 30 minutes of strong, persistent abdominal contractions without a delivery is an emergency, and more than 2 hours between kittens without myometrial contractions is an emergency. You do not average these numbers. You do not round down. They are the same rules your vet will use.
The data behind the 2-hour rule is specific. In a detailed French veterinary dataset of feline whelpings, the average interval between kittens was around 51 minutes, with a wide spread; total stage II typically averaged roughly 168 minutes (about 2.8 hours), but anything beyond 6 hours of total stage II is considered abnormal and is itself a reason to call. A note on rectal temperature: in dogs, breeders rely on the pre-labor temperature drop as a timing cue, and they rectal-check twice daily in the last week. In queens, I do not recommend that routine. Cats are sensitive to handling; repeated rectal checks add exactly the kind of stress that can suppress labor through psychological inertia. The primary timing tool in cats is the breeding-date log and the expected due date, not the thermometer.
| Stage or signal | Normal window | Call the vet if |
|---|---|---|
| Stage I (dilation) | 12 to 24 h, restlessness, nesting | >24 h with no stage II |
| Interval between kittens | Avg ~51 min, wide spread | >2 h with no contractions |
| Total stage II (all kittens) | Avg ~168 min (~2.8 h) | >6 h total |
| Active pushing | A kitten out within 15 to 30 min | >30 min of strong, unproductive pushing |
| Total gestation | 63 to 67 days typical | >70 to 71 days from first breeding |
| Kitten visible in canal | Delivered within 5 to 10 min | >10 min protruding, not advancing |
Uterine inertia is why most queens stall
When a feline labor goes wrong, the most common reason is not an obstruction. It is uterine inertia, the failure of the uterine muscle to contract effectively. Studies put this at up to 91% of feline dystocia cases. It is the quiet one. The queen does not look distressed; her uterus simply stops doing its job.
Inertia comes in two forms. Primary uterine inertia is when the uterus never builds effective contractions in the first place, often linked to hypocalcemia (low blood calcium), obesity, or extremes of litter size, either very small (one to two kittens, under-stimulating the uterus) or very large (overstretching the muscle fibers). Secondary uterine inertia is when the uterus starts well, pushes against something, and runs out of fuel. It fatigues and quits. The cause sits upstream, but the symptom, a stalled labor, looks identical in the moment.
Here is an important clarification for the vet side of the story. In the heat of an emergency, your vet will not try to differentiate primary from secondary inertia clinically. That distinction is useful in the textbook, not on the exam table. What your vet will do is two practical things: rule out mechanical obstruction with a radiograph (X-ray), which shows fetal number, size, and positioning, and assess fetal viability with ultrasound, which shows whether the kittens still have safe heart rates. Those two findings, obstruction yes or no, fetal distress yes or no, drive the medical-versus-surgical decision. That is why you transport fast: your vet needs those images to act.
| Type | What is happening |
|---|---|
| Primary uterine inertia | The uterus never produces effective contractions. Often linked to low calcium, obesity, or extreme litter size. |
| Secondary uterine inertia | Contractions begin, but the uterus exhausts itself pushing against an obstruction and quits. |
| Obstructive dystocia | A mechanical block (fetal oversize, malposition, narrow pelvis). Confirmed on radiograph (X-ray). |
| Psychological inhibition | A nervous queen voluntarily suppresses labor in a disturbed environment. Often responds to silence and seclusion. |
Breed matters more than cranial type alone
Breed shapes dystocia risk, and the pattern is less about flat faces than many breeders assume. A large Swedish insurance-database study (Holst and colleagues, 2017) looked at more than 200,000 insured queens across Sweden’s major breeds and counted how often dystocia showed up as an insurance claim in each one. They expressed the result as a dystocia risk index, a per-breed claim rate per 10,000 cat-years at risk. Higher number, more dystocia claims per insured queen. The Domestic Shorthair / Longhair population, the general cat, sits at the low end of the scale at about 7 and serves as the practical baseline you compare every purebred against.
The rankings that come out of that comparison surprise most breeders. The British Shorthair tops the list at 157, which is roughly 22 times the baseline risk of a Domestic Shorthair. Behind her sit the Oriental group (135), Ragdoll (102), Birman (101), and Abyssinian group (100), all four sitting at roughly 14 to 15 times baseline. Persians and Exotic Shorthairs, the textbook brachycephalic cases, land at a more moderate 38, about five times baseline. The Cornish Rex sits low at 34, the Maine Coon at 33, the Norwegian Forest Cat at 29. Cranial type alone does not explain this spread; maternal-fetal disproportion, conformational quirks, and maternal size each contribute, and they do not line up cleanly with flat faces versus long faces.
The practical message is the same either way: your breed matters, and the conversation to have about it is before breeding, not at 2 a.m. If your breed sits above 100 on the Holst index, your planning baseline is the high end of the curve, not the middle. If your breed sits below 40, you still prepare the same way; the baseline risk is lower, not zero. Bring your breed’s position on that scale into the pre-whelp visit and let it shape how closely you monitor late gestation, whether a scheduled pre-labor radiograph belongs in the plan, and whether a scheduled C-section deserves a discussion on the table.
| Breed or group | Dystocia risk index (Holst 2017) | Implication |
|---|---|---|
| British Shorthair | 157 | Top of the risk curve. Pre-whelp plan is mandatory. |
| Oriental group | 135 | High risk. Pre-whelp radiograph routinely. |
| Ragdoll | 102 | High risk. Staffed delivery window. |
| Birman | 101 | High risk. Pre-whelp plan with vet. |
| Abyssinian group | 100 | High risk. Pre-whelp plan with vet. |
| Persian / Exotic SH | 38 | Moderate risk. Pre-whelp radiograph if large single kitten. |
| Cornish Rex | 34 | Lower risk. Standard vigilance. |
| Maine Coon | 33 | Lower risk. Standard vigilance. |
| Norwegian Forest Cat | 29 | Low risk. |
| Domestic SH / LH | 7 | Baseline. |
The 2-Hour Rule and the 30-Minute Rule
The 2-hour rule between kittens
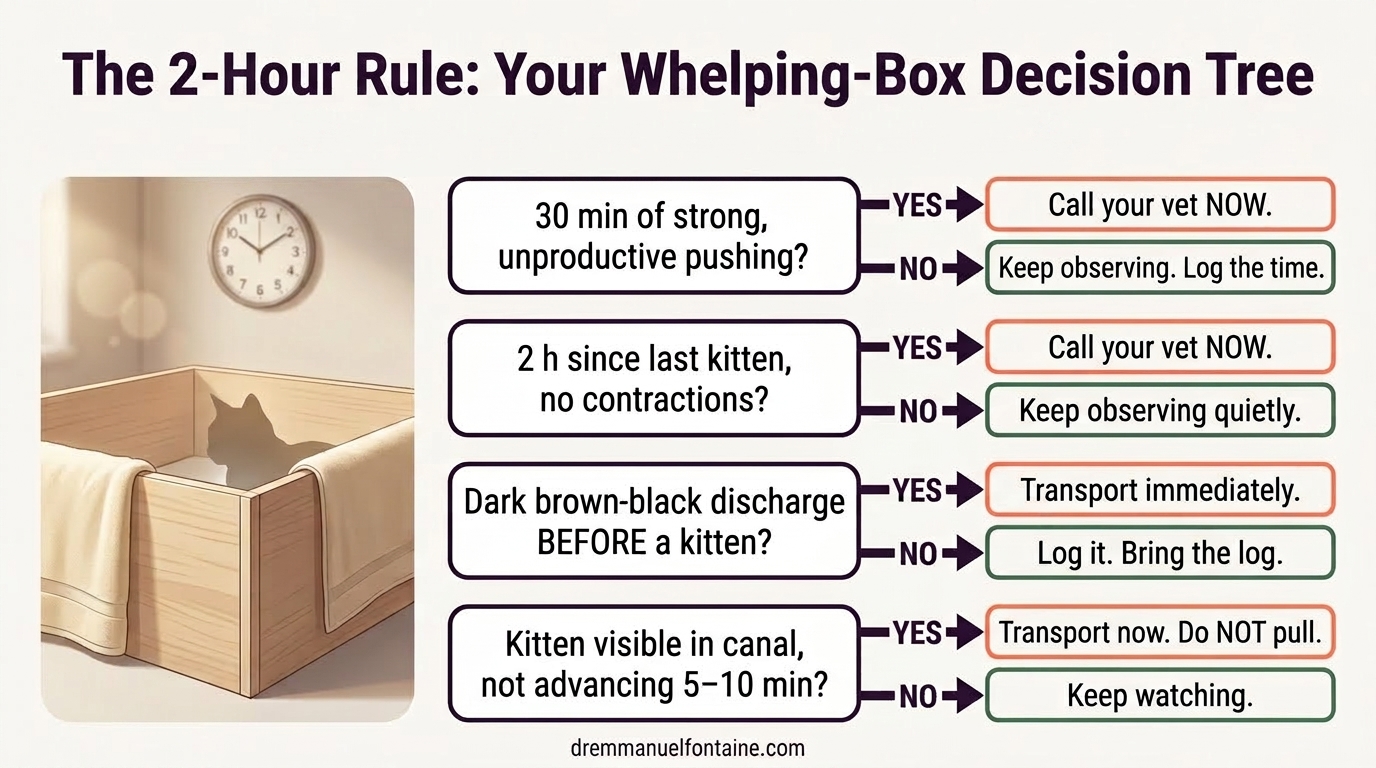
The 2-hour rule is the most reliable call you will make in the middle of the night. It is simple: if more than two hours have passed since the last kitten was delivered and your queen is not producing visible contractions, you are calling your vet. No exceptions. Not for a calm queen, not for a tired queen, not for a queen who looks fine.
The reason this rule is so strict is that the same quiet picture, a resting queen in a warm box, sits on top of very different biologies. She may genuinely be resting. She may also be in silent primary inertia or silent secondary inertia. You cannot tell from her face, and in the clinic your vet cannot tell either without a radiograph to rule out obstruction and an ultrasound to check the kittens. The 2-hour mark forces a call because, beyond that window, kitten survival in the litter still inside her drops fast.
Remember the inertia distinction from the earlier section. Before that call, no medication you might be tempted to buy online is safe. Oxytocin, in particular, is a veterinary-only drug that is actively dangerous if given against an obstruction or a calcium-depleted queen. You observe, time, and call. That is the whole protocol.
| Where you are on the clock | What you do |
|---|---|
| Last kitten <2 h ago, queen calm, contractions absent | Keep observing. Log time. Minimize interference. |
| 2 h since last kitten, no contractions | Call the vet now. Do not wait for contractions to restart. |
| 2 h since last kitten, queen appears exhausted | Call the vet. Prepare the carrier. Expect radiograph. |
| >3 h since last kitten, regardless of queen appearance | Transport now. Every additional hour costs kitten survival. |
| Known remaining kittens on radiograph, no progress in 2 h | Transport now. Confirmed retained kittens escalate fast. |
The 30-minute pushing rule and the phone call
The companion rule is the 30-minute pushing rule. If your queen is visibly straining, hard abdominal contractions, flank heaving, back arched, and has not produced a kitten within 30 minutes, you are on the phone. Not in an hour, not after one more push. Thirty minutes is the line. The risk here is mechanical: she may be pushing against an obstruction, and every minute of obstructed pushing worsens uterine fatigue and fetal oxygen debt.
When you call, give your vet four things and nothing else. The current time, the time of the last kitten, the duration of visible contractions in the current push, and the color and smell of any discharge. That is a 20-second call. Everything else, history, breed, litter size from the last scan, happens at the door, not on the phone. Your goal is to move faster, not to explain more.
The payoff of this call being short is that your vet is already thinking about a radiograph for obstruction, an ultrasound for fetal viability, and operating room availability while you are still in the car. That lead time changes outcomes.
| What you see or feel | What you say on the phone |
|---|---|
| 30 min strong pushing, no kitten | “Thirty minutes of hard contractions, no delivery. On our way.” |
| 2 h since last kitten, no contractions | “Two hours since last kitten, no contractions. On our way.” |
| Dark brown-black discharge, no kitten delivered yet | “Dark brown-black discharge before the first kitten. On our way now.” |
| Kitten protruding, not advancing for 5 to 10 min | “Kitten visible, not advancing for X minutes. On our way.” |
| Queen collapsed, trembling, or unresponsive | “Queen is collapsed. We are leaving now. Arriving in X minutes.” |
Vaginal discharge: the colors that change your night
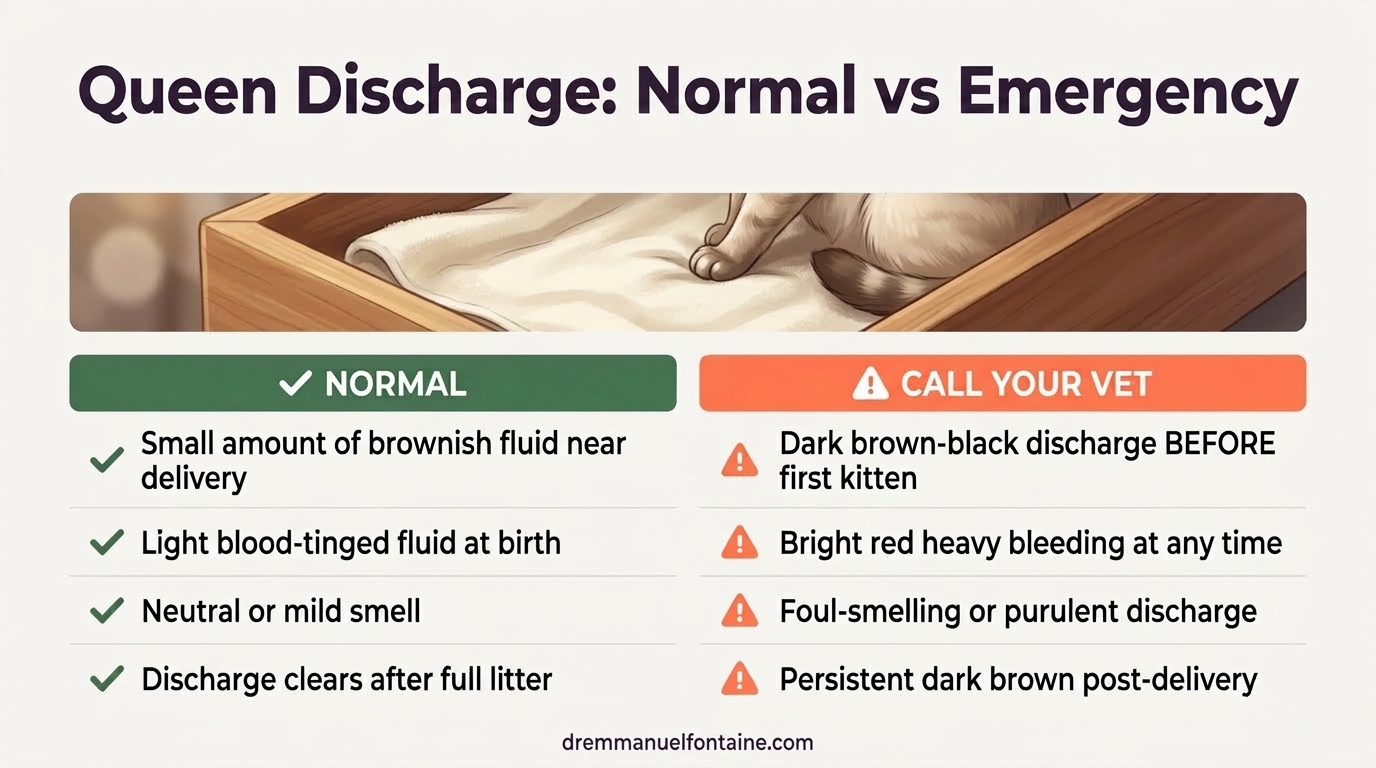
Discharge color is the earliest visible signal you have, and it beats every soft sign. A small amount of brownish fluid around the time of an actual delivery is within the expected range for cats. What is never normal, and what you put on the wall, is one of three specific patterns, each of them a reason to transport.
Dark brown-black or heavily brown discharge before the first kitten is born is a red alert. That color is the feline placental pigment: a natural dark-brown pigment stored along the edge of the feline placenta that is released when the placenta detaches from the uterine wall. Seeing it before a kitten has been delivered means a placenta has separated ahead of its kitten, which means the kittens on that side are losing their oxygen supply. If you ever see this before a kitten is out, you are already late; go now. Bright red heavy bleeding at any point suggests genital tract trauma or hemorrhage. Also go now. A foul-smelling or purulent discharge signals infection or, more ominously, a retained decomposing fetus and needs urgent assessment.
A small serous or lightly blood-tinged fluid around the time of a delivery can be normal. What is never normal is dark brown-black discharge before a kitten is delivered, heavy red bleeding at any time, or a foul smell. Those are the three you put on the wall. Everything else, you log, and you bring the log.
| Red flag | What it may mean | Action |
|---|---|---|
| Dark brown-black discharge before a kitten | Premature placental separation | Transport immediately |
| Bright red, heavy bleeding | Genital tract trauma or hemorrhage | Transport immediately |
| Foul-smelling or purulent discharge | Infection or retained decomposing fetus | Urgent vet assessment |
| >30 min strong contractions, no kitten | Obstruction or exhaustion | Transport immediately |
| >2 h between kittens | Primary or secondary uterine inertia | Transport immediately |
| Weak straining >2 to 4 h, no kitten | Inadequate uterine tone | Transport immediately |
| Gestation >70 to 71 days, no labor | Silent complete primary inertia | Vet assessment today |
| Total stage II >6 h | Abnormally prolonged whelping | Vet assessment today |
| Queen collapsed, tremoring, pale gums | Maternal crisis (shock, bleed, hypocalcemia) | Emergency transport |
| Queen ignoring delivered kittens | Maternal distress or illness | Call vet; warm and care for kittens |
What You Keep Ready Before Labor Begins
The queening box and the 1-to-2-week pre-acclimation
Most breeders focus on supplies. The single most undervalued piece of preparation is not a supply, it is time. A queen who enters labor in a new, unfamiliar box is a queen at risk of psychological inhibition, where nervousness or disturbance makes her voluntarily suppress contractions. This can trigger the quiet version of primary inertia even in an otherwise healthy cat.
The fix is cheap. Set up the queening box, in its final location, ideally one to two weeks before the due date. Two weeks is the target when your queen is new to the space, particularly nervous, or a first-litter queen; seven days is the absolute minimum. Let her sleep in it, eat near it, nest in it, or ignore it if she wants to; do not move it and do not clean it aggressively. By the time she enters stage I, the box smells like her, and her nervous system has nothing to argue with.
Once labor begins, your observation discipline is the second half of this tool. Observe from a distance, log silently, and resist the urge to hover, pat, or talk. Your calm is part of her protocol. This is also the reason I do not recommend twice-daily rectal temperature checks in queens: the checking itself is the stressor, and the stress is the very thing that can stall a labor you are trying to monitor.
| Item | Why it matters |
|---|---|
| Queening box, set up 1 to 2 weeks pre-due | Prevents psychological inhibition of labor |
| Absorbent bedding (towels, sheets, newsprint) | Traction for kittens, easy change between deliveries |
| Written breeding-date log + expected due date | A gestation >70 to 71 days is itself a vet trigger |
| Accurate gram scale | Tracks post-delivery weight; a falling newborn triggers a vet call |
| Microwaveable heating pad or beanie (never hot water bottles) | Safe neonatal warmth; hot water bottles puncture on claws |
| Clean carrier, ready by the door | Transport time counts in minutes, not hours |
| Printed red-flag card on the box | Removes guesswork at 3 a.m. |
| Pre-whelp radiograph appointment (late gestation) | Counts kittens; flags oversized singletons |
| Your vet’s emergency number pre-dialed | Cuts your call latency by 30 seconds at the worst moment |
The queen’s readiness profile
Not every queen enters labor equally prepared. Body condition, breed, and litter size from the pre-whelp radiograph all change her risk profile, and they change yours. An overweight queen carries more than extra weight; she carries fatty infiltration of the uterine muscle, which is one mechanism behind primary inertia. A very small litter may not produce enough stretch on the uterus to trigger full labor; a very large one may overstretch and exhaust it.
The pre-whelp radiograph, taken late gestation, gives you and your vet two numbers that matter: the kitten count and a rough sense of whether the largest kittens look disproportionate for the pelvis. If your queen is in a high-risk breed group and the radiograph flags a large single kitten, that is the moment to plan, not the moment to improvise.
Remember the breed table from the first section. You use it here again as a conversation prompt with your vet, not as a decision tool on its own. A British Shorthair with a small litter of big kittens is a very different planning problem than a Domestic Shorthair with a typical spread, and the plan is made at the pre-whelp visit.
| Readiness signal | What it suggests | Conversation with your vet |
|---|---|---|
| Obese queen (BCS 8 to 9 of 9) | Higher primary inertia risk | Pre-breeding weight plan, monitored gestation |
| Very small litter (1 to 2 kittens) | Oversized single kitten risk | Radiograph; consider scheduled C-section |
| Very large litter (>6 kittens) | Uterine overstretch and fatigue risk | Prepare for secondary inertia |
| High-risk breed group (BSH, Oriental, Ragdoll, Birman, Abyssinian) | Index >100 in Holst 2017 data | Pre-whelp radiograph; plan surgical option |
| Previous dystocia in this queen | Higher recurrence risk | Pre-whelp visit; staffed delivery window |
| No labor by day 70 to 71 | Possible complete primary inertia | Vet assessment same day, not tomorrow |
What happens when you reach the clinic
When your queen is on the clinic table, your job shifts. You are not making the drug decision. Oxytocin is a veterinary-only medication and it is never administered at home, by breeders, under any circumstances. Your role is to get her there fast and give your vet the clean history. Everything else is on the vet’s side of the table.
Here is what your vet will do when you arrive, so you know what to expect and why the call has to be short. First, a radiograph to rule out mechanical obstruction, show fetal number, and flag disproportion. Second, an ultrasound to read fetal heart rates and judge viability. Those two findings shape the medical-versus-surgical decision. If there is no obstruction and the kittens still have safe heart rates, your vet may choose low-dose medical management under direct supervision. If there is obstruction, or if fetal heart rates have dropped, surgery is the safer answer.
One part of that medical-management decision is worth understanding, not for you to influence it, but so you can follow your vet’s reasoning. Smooth muscle needs calcium to contract. When medical management is chosen, your vet will usually address calcium before or alongside any low-dose oxytocin, because oxytocin given to a calcium-depleted queen often does very little. Medical management has a strict ceiling: if one or two low-dose attempts at the clinic do not produce a kitten, medical management is over and surgery is the right answer. A vet moving to C-section after two oxytocin attempts is not giving up. She is following the data.
| Clinical situation | What your vet does, and why |
|---|---|
| Arriving with a stalled queen | Radiograph first (obstruction? fetal count?), then ultrasound (fetal HR) |
| No obstruction, stable fetal HR | Medical management becomes an option under vet supervision |
| Confirmed obstruction on X-ray | No oxytocin. Surgery is safer for queen and kittens |
| Medical management selected | Calcium typically addressed before or with low-dose oxytocin |
| Two oxytocin attempts, still no delivery | Medical management is over. Surgery now |
| Fetal heart rate below 180 bpm on ultrasound | Fetal stress. Surgery clock starts |
| Fetal heart rate below 140 to 160 bpm | Severe hypoxia. Surgery now, no more medication |
The Signs That Tell You the Next Minute Matters
When a kitten is too big to pass
Obstructive dystocia is less common than inertia, but when it is happening, the window is shorter. The clue is the combination of strong, productive-looking contractions with no forward progress, sometimes paired with a kitten visible in the canal that does not advance. Your queen is working, but the physics is wrong.
You cannot confirm fetal oversize at home, and you should not try. Home palpation or any attempted internal examination belongs to your vet. What you can do is recognize the pattern, transport fast, and let the radiograph do the confirming. The signal is visible effort without delivery, and sometimes a partially protruding kitten that is not advancing within five to ten minutes.
The temptation to pull is strong. Do not pull. Traction on a trapped kitten from the outside tears tissues and rarely solves the underlying geometry. Transport. The operating room solves this problem cleanly.
| Signal | What it suggests |
|---|---|
| Strong contractions, zero forward progress | Mechanical obstruction; consider fetal oversize |
| Kitten visible, stuck >5 to 10 min | Fetal malposition or disproportion |
| Very small litter (1 to 2 kittens) on radiograph | Single kitten may be oversized for canal |
| High-risk breed, first delivery | Elevated disproportion risk at baseline |
| Queen tiring rapidly on productive pushes | Secondary inertia developing from obstruction |
What to watch for after a dystocia is resolved
A resolved dystocia is not a finished problem. Whether your queen delivered the rest of her litter medically or surgically, the next 24 to 48 hours carry their own risks, and your observation work shifts from labor signs to maternal and neonatal recovery. You are the one spending the most time at the box; you are the one who will notice when something changes.
For the queen, watch for fever (rectal temperature above 39.4 °C (103 °F) if your vet has asked you to check it, done once rather than the twice-daily dog routine), lethargy that does not resolve in a few hours, refusal to nurse, a foul-smelling discharge, and any sign that she is not settling with her litter. For the kittens, the monitoring points are weight at each feeding check, temperature, activity when disturbed, and nursing behavior. A falling kitten weight in the first 24 hours is itself a vet call, not a ‘wait and see’.
This is where a printed monitoring log earns its keep. Log every observation for 48 hours. When you call your vet with concerns, the log is the difference between a guessing phone call and a useful one.
| Monitoring point | Trigger for a vet call |
|---|---|
| Queen rectal temperature (if requested by vet) | >39.4 °C (103 °F) or trending upward |
| Queen behavior | Lethargy >4 h; not settling with litter |
| Queen vaginal discharge | Foul smell, heavy red, or persistent dark brown |
| Queen nursing | Refusing kittens; milk not letting down |
| Kitten weight | Any kitten losing weight in first 24 h |
| Kitten temperature | Cold to the touch or cannot self-maintain |
| Kitten activity | Limp, silent, or not rooting to nurse |
Every minute matters: timing and survival
Here is the hardest truth about feline dystocia, and the reason the 2-hour rule and 30-minute rule exist in their current unforgiving form. Kitten survival in dystocia cases is time-sensitive in a way that maternal survival is not. Queens usually survive dystocia. Kittens usually do not, and the ones that do tend to be the ones delivered fastest.
Medical management succeeds in roughly 37% of feline dystocias under the right conditions, always at the clinic, always under veterinary supervision. The other 63% need surgery, and the surgery the queen gets at the second hour is different from the surgery she gets at the fourth. In the first two hours, your vet has a stable queen, oxygenated kittens, and time to plan anesthesia. By hour four, fetal heart rates have often dropped, the queen is dehydrated and exhausted, and kitten survival numbers fall sharply.
You do not need a study to internalize this. The drill is: recognize, call, transport. That triplet is the entire high-leverage part of your job. Your vet handles the rest. Keep the flowchart on the wall, the carrier by the door, and your vet’s number in your thumb.
| Intervention timing | Outcome pattern |
|---|---|
| Within 2 h of stall | Best litter survival; widest vet options |
| 2 to 4 h after stall | Falling litter survival; C-section probability rises |
| >4 h after stall | Sharp drop in kitten survival; queen fatigue climbs |
| Overnight wait, intervention next morning | High kitten loss rates regardless of queen outcome |
| Transport initiated before the 2 h mark | Often keeps medical management on the table at the clinic |
Conclusion
Feline dystocia rewards two things: prepared breeders and fast decisions. Everything else, the radiograph, the ultrasound, the calcium, the oxytocin, the decision to operate, belongs on your vet’s side of the table. Your side is simpler. You set up the quiet box one to two weeks early, you keep a clean breeding-date log, you log the times once labor begins, and you follow two rules without bargaining: 30 minutes of hard, unproductive pushing, or 2 hours between kittens, means you call.
The flowchart on your wall is the tool that saves you from negotiating with yourself at 3 a.m., when every instinct will tell you to wait five more minutes. Your queen is stoic. Her uterus, if it has stopped, will not announce itself. Your clock and your phone are the two instruments that catch what her behavior hides.
This post gives you the rules. Your vet gives you the rescue. Between the two of you, the litter in front of you tonight has the best chance it can have. That is the partnership pediatric reproduction was built on, and it is the one that wins nights like the one you are reading this for.

Thank you Dr Emmanuel. This reinforced so much I learned over the years. I wish I had known all of this 25 years ago.
LikeLike