🇫🇷 Lire en Français | 🇪🇸Leer en Español | 🇧🇷Leia em português
Walk into a modern human neonatal intensive care unit and you may see something quietly extraordinary. Premature babies receive named bacterial strains, prescribed by a neonatologist, with the same discipline used for any other medication.
This is the part of human neonatology that has matured the most in the last decade. It is also the part most often misread by people outside the unit.
The shift is not that babies suddenly get probiotics. The shift is that the field stopped saying “probiotics” and started naming strains, naming doses, naming manufacturers, and naming the exact patient profile each strain was tested in.
A 2023 European position paper put that line in writing. A 2023 safety alert from the United States Food and Drug Administration drew it again, much harder.
I follow this file closely. As a veterinarian working with breeders, I am not asking whether human protocols can be lifted wholesale into the whelping or queening box. They cannot.
My question is more specific: what can we learn from human neonatal medicine, and what fragments of that thinking could one day inform how we support newborn puppies and kittens?
TL;DR
- The biggest shift in human neonatology is moving from the word “probiotic” to the strain name. Same genus, different strain, very different result.
- A 2023 European position paper named a small set of strains with strong evidence in preterm infants. The same year, a fatal contamination event reframed the safety conversation around manufacturer quality and lot testing.
- Mechanism crosses species. Strains, doses, and regulatory frames do not. What works in a 28-week preterm infant is not what works in a five-day-old puppy or kitten.
- Dog and cat probiotic data in newborns is thin today. There are promising research signals in adult and weanling animals, but neonatal trials remain few.
- The transferable lesson, even now, is the strain-first mindset: pick the strain, then the manufacturer, then the conversation with your veterinarian.
What human neonatology has actually figured out about probiotics
Strain identity is the conversation, not “probiotic”
Most breeders reach for the word probiotic the way they reach for the word antibiotic: as if it referred to a single category that behaves the same way across products. It does not.
Two products on the same shelf can both be labelled probiotic and contain bacteria from the same genus, and yet behave like different drugs in the body.
Human neonatology spent two decades learning this the hard way. The pivotal trials are not Lactobacillus trials or Bifidobacterium trials.
They are strain trials: a specific bacterial strain, with a specific identifier, grown by a specific manufacturer, given at a specific dose, in a specific patient profile.
Swap the strain for a sibling within the same species and the outcome can change by half. Genus is a family. Strain is the individual.
This is the single most important transformation I want a breeder to take from this article. If you remember nothing else: when you read the word probiotic on a label, you are reading a category, not a product.
Ask the strain name. If the label cannot give you one, you are not looking at a probiotic in the modern clinical sense.
| Same genus, different strain | Where the difference shows up | Why this matters for thinking about newborns |
|---|---|---|
| Bifidobacterium infantis EVC001 vs. another B. infantis strain | Stable colonization vs. transient passage through the gut | A label can say B. infantis and still not deliver the strain that was studied |
| Lactobacillus rhamnosus GG vs. another L. rhamnosus | Documented effect on diarrhea outcomes vs. unknown effect | Strain identifiers (the letters and numbers after the species) carry the evidence |
| A multi-strain blend of named strains vs. an unnamed multi-strain blend | Pooled trial signal vs. no published trial behind the blend | Marketing language can copy the words but not the science |
| A research-grade strain vs. the same strain after manufacturing changes | Original effect vs. unverified effect | Strain identity is preserved only when the manufacturer verifies it lot by lot |
The short list of strains with the strongest evidence in human neonates
In 2023, the European Society for Paediatric Gastroenterology, Hepatology, and Nutrition issued an updated position paper on probiotics in preterm infants. It did not endorse probiotics in general.
It named specific strains with the strongest evidence for reducing two outcomes: necrotizing enterocolitis (a severe inflammatory disease of the immature gut that can destroy intestinal tissue in the first weeks of life), and all-cause mortality in the unit.
The named strains are a short list. Bifidobacterium infantis EVC001, Lactobacillus rhamnosus GG, and a handful of multi-strain combinations that pair Bifidobacterium and Lactobacillus species with Streptococcus thermophilus.
Each name carries a specific evidence package. Strip the strain identifier away and the evidence does not travel with it.
None of these strains were tested in newborn puppies or kittens. And none should be assumed to behave the same way if they were.
The reason to know this list is not to replicate it in a whelping or queening box. The reason is to see, concretely, what strain-level evidence looks like when it has actually been built.
| Strain or combination (human neonatal evidence) | What the strain identity actually buys you |
|---|---|
| Bifidobacterium infantis EVC001 | Stable colonization of the preterm infant gut and lower inflammatory markers, in trials that tracked this exact strain |
| Lactobacillus rhamnosus GG | Decades of human pediatric data, with broad use across multiple gut indications |
| Multi-strain combinations of Bifidobacterium, Lactobacillus, and Streptococcus thermophilus (study-defined formulations) | Pooled trial data showing reduced mortality and lower necrotizing enterocolitis risk |
| Lactobacillus reuteri (selected strains) | Mixed results in preterm trials; conditional support depending on strain and population |
| Yeast-based products (Saccharomyces boulardii lineages) | Useful in some adult human gut indications but treated cautiously in fragile neonates |
Why manufacturer quality became part of the safety story
In September 2023, the United States Food and Drug Administration issued a public warning. A preterm infant had died from sepsis traced to a probiotic product contaminated with Cronobacter sakazakii, a pathogen sometimes found in dry food ingredients.
The case did not invalidate the strain evidence from the 2023 European position paper. It clarified a different question: what stands between a live bacterial product and a fragile newborn?
That short list is the manufacturer’s quality system. Strain identity verification, lot testing, contamination screening, cold chain control, and clinical supervision are the actual safety story behind any modern probiotic that a clinician feels comfortable putting near a newborn.
Two products with the same strain on the label can sit on opposite ends of this quality spectrum. The label cannot tell you which is which.
The lesson for breeders is not to fear probiotics. The lesson is to look at the manufacturer the way you would look at a stud dog or a queen on paper: track record, transparency, third-party testing, willingness to answer questions.
A company that cannot tell you the strain identifier, the lot testing process, and the trial history of its product is not a partner you want anywhere near a neonatal litter. That standard holds even if you only ever use that product in adult animals in your home.
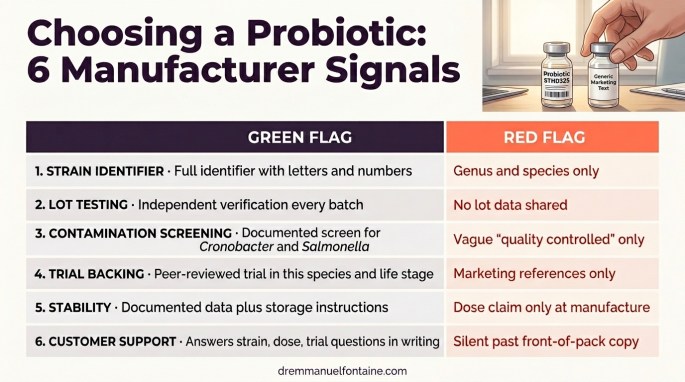
| Manufacturer signal | Green flag | Red flag |
|---|---|---|
| Strain identifier on the label | Full identifier with letters and numbers (e.g., a named research strain) | Genus and species only, or marketing-only branding |
| Lot testing and CFU verification | Independent verification on every batch, with results available | No lot data; CFU only at manufacture, not at end of shelf life |
| Contamination screening | Routine screening for organisms like Cronobacter and Salmonella with documented method | No statement on screening; vague “quality controlled” phrasing |
| Published trial backing the strain | Peer-reviewed trial in the species and life stage of interest | Marketing references only; mechanism speculation rather than outcomes |
| Cold chain and stability | Documented stability data; clear storage instructions | No stability data; dose claim refers only to time of manufacture |
| Customer support | Will answer strain, dose, and trial questions in writing | Cannot or will not answer beyond the front-of-pack copy |
The biology that crosses the species line
Colonization resistance during the first weeks
A newborn intestine is a blank canvas. The microbes that arrive first occupy the mucosal real estate, set the local pH, and crowd out late-coming pathogens.
This effect is called colonization resistance, and it is one of the most conserved pieces of biology across mammals.
Recall the strain Bifidobacterium infantis EVC001 from the section above. In preterm human infants, it has been shown to occupy that niche so completely that the abundance of antibiotic-resistance gene markers in the stool drops measurably.
The biology behind that result is not human-specific. It is the biology of any newborn gut.
Newborn puppies and kittens build their early gut community through the same mechanism. It is fed by maternal vaginal flora at birth, by skin bacteria during licking, and by the live bacteria that arrive in colostrum and milk.
The first three weeks are the high-leverage window in both species. After that, the community structure becomes harder to reshape with anything short of major disruption.
| Stage | What happens in the newborn gut | Why it matters for puppies and kittens |
|---|---|---|
| Birth | A near-sterile gut meets the first wave of maternal microbes | Birth route, maternal hygiene, and dam or queen health all shape the starter culture |
| First feeding | Colostrum delivers immunoglobulins plus prebiotic sugars that feed pioneer species | Missed colostrum is missed microbiome seeding, not just missed antibodies |
| First 21 days | Pioneer species occupy the lining, set local pH, and begin training the immune system | This is the window where the microbiome is most plastic and most fragile |
| Weaning transition | The community shifts toward a more adult-style diversity | Diet changes here can either consolidate or destabilize the work of the first three weeks |
| Antibiotics or illness | A window opens for opportunists to expand | These are the moments where probiotic thinking has the most theoretical leverage |
How the gut and immune system mature together in the first weeks
A newborn animal’s immune system is not just inexperienced. It is physically still being built.
Along the inside of the small intestine, clusters of immune-training tissue, sometimes called intestinal lymphoid patches or Peyer’s patches, expand and mature in direct response to the bacteria they meet. Think of them as classrooms in the gut wall, where the immune system learns what to ignore and what to attack.
This education window is short and decisive. In altricial neonates like puppies and kittens, the same biology unfolds on a fast clock.
Live bacteria interact with the cells lining the gut, immune scouts in the gut wall sample what is there, and the body calibrates its baseline tolerance for the months and years ahead. Disturb that conversation early, and the consequences can echo well past the neonatal period.
This is why the question of probiotics in newborns is never simply “do they help digestion?” It is also: do they shape the immune system the gut is wiring itself into for the rest of the animal’s life?
The answer in human neonates is increasingly yes, for specific strains. The answer in puppies and kittens is largely an open research question.
| Job the live bacteria do | What it looks like on the inside | Why a breeder should care |
|---|---|---|
| Colonization resistance | Pioneer species claim space and lower local pH | Crowds out organisms like enterotoxigenic Escherichia coli and Clostridium perfringens |
| Barrier maturation | Tight junctions between gut cells strengthen; mucus production increases | Reduces leakage of bacteria from gut into bloodstream in fragile neonates |
| Immune training | Lymphoid patches and regulatory immune cells calibrate to the new environment | Lays the foundation for adult tolerance to food and environment |
Where the puppy and kitten gut differ from the human preterm gut
Mechanism travels. Strains, doses, and timing do not.
The puppy gut differs from the human preterm gut in three ways that matter. The dominant early bacterial families are different.
The moment when the gut stops absorbing whole proteins, called gut closure, happens dramatically faster in puppies than in human infants. And neonatal dose-finding studies in puppies are still few.
Kittens compress the timeline even further. Gut closure in kittens occurs around 16 hours after birth, compared with about 24 hours in puppies and a more gradual process measured in days for human infants.
That single number reshapes the timeline of any colostrum-related or microbe-related intervention in feline neonates. The window where what enters the gut can still cross the lining as a whole molecule, including immunoglobulins and possibly some live bacteria, is extraordinarily narrow.
Cat-specific neonatal probiotic data is even thinner than dog data. The few studies on adult cats and selected Enterococcus or Lactobacillus strains do not translate cleanly to kittens.
Queen-to-kitten microbiome transfer dynamics still need a lot more research before they can support recommendations. When in doubt with a litter of kittens, the conservative position is to lean harder on the maternal side of the equation: queen health, colostrum, hygiene, and your veterinarian’s eye on the litter.
| Feature | Human preterm infant | Newborn puppy | Newborn kitten |
|---|---|---|---|
| Maturity at birth | Often 24 to 36 weeks gestation | Full term, altricial | Full term, altricial |
| Early dominant microbes | Enterobacteriaceae, then Bifidobacterium with EVC001 if given | Clostridium, Lactobacillus, Bifidobacterium | Lactobacillus, Bifidobacterium, Bacteroides |
| Gut closure timing | Gradual, days to weeks | Around 24 hours | Around 16 hours |
| Strain evidence base | Robust for a short list of strains | Limited neonatal data; adult and weanling signals | Very limited neonatal data overall |
| Primary clinical concern | Necrotizing enterocolitis, sepsis | Fading puppy, neonatal diarrhea, sepsis | Fading kitten, neonatal diarrhea, sepsis |
What this could mean for newborn puppies and kittens, eventually
Promising avenues already being studied
This is the section I find most exciting. It is also the section where I have to be most disciplined.
Veterinary research has not produced anything that resembles the named-strain, named-dose, named-population package that exists in human neonatology. What it has produced is a growing set of signals, in adult and weanling dogs and cats, that point to where neonatal research could realistically land in the coming years.
A few specific avenues are worth naming. Dam and queen supplementation in late gestation and lactation, with selected strains, to enrich the maternal microbiome that the neonates inherit at birth and through colostrum and milk.
Targeted use during stress windows, such as weaning or after antibiotic courses given to the dam or queen, where the early community is at its most disturbed. Strain-specific support around episodes of neonatal diarrhea, under direct veterinary supervision, in litters where the loss profile justifies the conversation.
Pre- and postbiotic ingredients in maternal diets during gestation and lactation, an area already represented in some commercial reproduction diets. Probiotic support after antibiotic exposure in either the dam or the neonates, mirroring an idea already in active use in human neonatology.
None of these avenues are protocols today. Each of them is a research direction with enough early signal that I would not be surprised to see clearer guidance over the next five to ten years.
That timeline is not a reason to wait passively. It is a reason to develop the strain-first habit now, in adult animals in your home, so that when neonatal guidance does arrive you are already fluent in the language it will be written in.
| Possible future application | What human or veterinary research currently suggests | Where the evidence sits today |
|---|---|---|
| Dam and queen supplementation in late gestation and lactation | Maternal microbiome shapes neonatal microbiome through birth, licking, colostrum, and milk | Some published signals in dogs and other species; specific neonatal-outcome trials still scarce |
| Probiotic support during weaning stress | Weaning is a microbiome-disrupting event; strain-specific support studied in production species | Translatable in principle; neonatal-stage dog and cat trials still limited |
| Strain-specific use around neonatal diarrhea episodes | Targeted strains studied in adult and weanling diarrhea cases | Used clinically in some practices today; rigorous neonatal trials still pending |
| Pre- and postbiotic ingredients in maternal diets | Already present in some commercial reproduction diets | Marketed today; outcome data continues to grow |
| Probiotic use after antibiotic exposure in dam or neonate | Antibiotic disruption is a high-leverage moment in human neonatology | Veterinary supervision essential; strain-specific dosing data in puppies and kittens still needed |
Where the dog and cat evidence base still has gaps
Honesty about the gaps protects you from products that overstate them. Three categories of evidence are missing or thin in newborn puppies and kittens.
Strain-level dose-finding studies in the first three weeks of life. Long-term follow-up beyond the immediate neonatal period. And independent verification that what is sold under a name is biologically the same as what was studied under that name.
This is not a criticism of veterinary research. It is a description of where the field actually is.
Designing and running neonatal trials in any species is hard. Doing it in altricial species like puppies and kittens, where neonatal numbers are smaller and litters are family units rather than individual subjects, is harder still. The field is moving. It just is not finished.
Knowing where the gaps live is what allows me to read a probiotic label honestly. If a product claims neonatal benefits in puppies or kittens with strong language and weak citations, the gap, not the science, is doing the marketing work.
That is a useful filter to bring with you the next time a label catches your eye.
| Evidence category | State today in newborn dogs and cats |
|---|---|
| Strain-level dose-finding in the first three weeks of life | Sparse; most data from older puppies and kittens or from adults |
| Long-term follow-up beyond the neonatal period | Limited; most trials end at weaning or earlier |
| Independent strain identity verification on commercial products | Inconsistent; varies sharply by manufacturer |
| Breed-size and life-stage adjustments | Rare; most veterinary probiotic labels do not distinguish by breed size or life stage |
| Safety thresholds in altricial neonates | Largely inferred from adult and weanling data; explicit neonatal safety studies remain few |
Why the strain-first mindset matters even before the protocols arrive
Even today, every adult dog and cat probiotic decision a breeder makes can be made through a strain-first lens. That habit is not a luxury for the future.
It is the daily practice that turns a passive consumer into an informed one. This holds whether the product is for a four-year-old stud dog with loose stools after a show, or a five-year-old queen recovering from an antibiotic course.
The strain-first habit also reshapes the conversation with your veterinarian. Walking in with “I want to try a probiotic” puts the entire decision on the vet.
Walking in with “I have read about this specific strain in this specific situation, what do you think?” turns the appointment into a partnership. The first question is open-ended and shopping-list shaped. The second is a clinical conversation.
If or when neonatal probiotic guidance for dogs and cats does emerge in a more concrete form, the breeders who will use it best are the ones who already speak strain.
You can become one of them right now, with the products you already see on shelves, by simply changing the question you ask first.
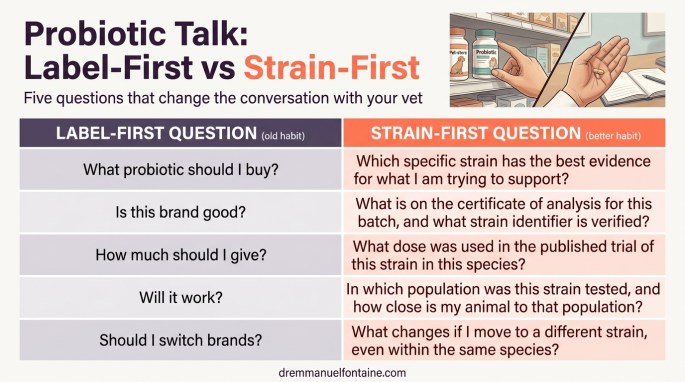
| Label-first question (old habit) | Strain-first question (better habit) |
|---|---|
| “What probiotic should I buy?” | “Which specific strain has the best evidence for what I am trying to support?” |
| “Is this brand good?” | “What is on the certificate of analysis for this batch, and what strain identifier is verified?” |
| “How much should I give?” | “What dose was used in the published trial of this strain in this species?” |
| “Will it work?” | “In which population was this strain tested, and how close is my animal to that population?” |
| “Should I switch to another brand?” | “What changes if I move to a different strain, even within the same species?” |
What a breeder can do today
The strain-first conversation with your veterinarian
Probiotic decisions in puppies and kittens are veterinary decisions. That phrasing is deliberate, and it mirrors the human neonatal model where the neonatologist signs off on every dose.
Recall the 2023 safety event from the manufacturer-quality section above. The lesson there was supervision, not abandonment. The same logic applies in your whelping or queening box.
Your role is to organize the evidence about your specific litter, your specific dam or queen, and your specific breeding context. Then ask informed questions.
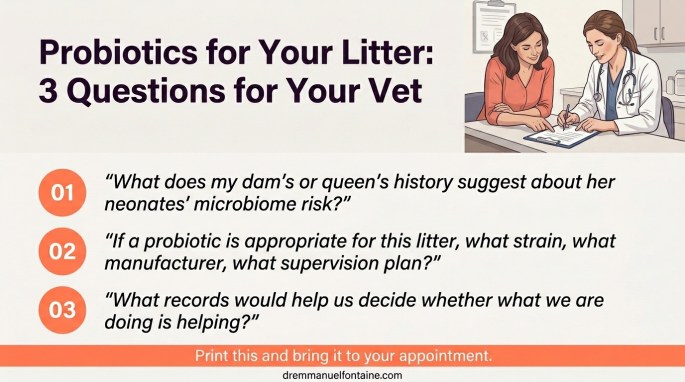
Three questions are worth bringing to your appointment. Each one opens a clinical conversation.
First, what does my dam’s or queen’s history suggest about her neonates’ microbiome risk? Second, if a probiotic conversation is appropriate for this litter, what strain are we talking about, what manufacturer, and what supervision plan?
Third, what records would help us decide whether what we are doing is helping?
Notice what these questions do. They keep your veterinarian as the decision partner, not the gatekeeper. They also keep you out of the trap of arriving with a product in mind.
The conversation is the value. Whether it ends in a probiotic decision or in a different intervention entirely, you will walk out with a clearer plan than you walked in with.
| What to bring to your vet appointment | Why it helps |
|---|---|
| Maternal history (antibiotic use, prior litters, illness) | Sets the microbiome context for this specific dam or queen |
| Litter records (weight curves, stool consistency, neonatal events) | Provides a baseline against which any change can be measured |
| A specific strain you have read about, with the source | Lets your vet evaluate the evidence and the product chain together |
| Any prior probiotic use in adult animals in the home | Reveals exposure history and tolerance |
| Your goal in your own words (less diarrhea, fewer fade neonates, calmer weaning) | Clarifies what you and your vet are actually trying to change |
Records that turn observation into evidence
A breeder who records is a breeder who can act on what she sees. A human neonatal unit runs on numbers: heart rate, feeds, weights, stool patterns.
The whelping or queening box can run on a smaller, more disciplined version of the same idea. Daily neonatal weights, stool quality notes, latch and nursing observations, and any antibiotic exposure in the dam or queen are the veterinary evidence backbone.
When something seems off in a litter, the difference between “I think the puppies are loose” and “day 4 weights flat, stool consistency 2 of 4 on three of seven puppies, dam on amoxicillin from day 1” is the difference between speculation and a clinical conversation.
The records are what allow your veterinarian to interpret a probiotic question with care. Whether the answer ends up being yes or no, the conversation is anchored.
This is also where breeders quietly change the field. Litter records, kept consistently across generations, are the kind of data that makes future veterinary trials possible.
Every well-kept whelping or queening journal contributes to the evidence base that newborn puppies and kittens, both species, deserve.
| Field to record | What to capture |
|---|---|
| Date and age in days | The anchor for every entry |
| Weight in grams | Daily; calculate gain or loss from the prior 24 hours |
| Stool consistency | Describe in plain words (firm, formed-soft, soft-unformed, loose, watery), per neonate where possible |
| Latch and nursing | Yes or no, plus a brief note on vigour |
| Maternal medications | Any drug given to the dam or queen, with date and reason |
| Notable events | Cold neonate, separation from litter, vet visit, dewclaw removal, anything outside routine |
How to evaluate any probiotic product, even today
Even before any neonatal guidance for puppies and kittens arrives, you will keep meeting probiotic products. In adult dogs and cats, around antibiotic courses, around dietary changes, around show stress, around weaning.
Every one of those products is a chance to practice the strain-first mindset.
The questions to ask the manufacturer are not exotic. They are the same questions a clinician would ask before signing off on any live bacterial product near a fragile patient.
If the manufacturer cannot answer them, that is itself the answer. Move on, and keep looking for a company that treats your animals the way it treats its data.
This is the manufacturer-quality conversation from earlier in this article, brought home to your kitchen counter. None of it is about being suspicious of probiotics. It is about being respectful of the biology.
Live bacteria can do real work in a newborn or adult gut. The companies that take that work seriously are easy to find once you know what to ask.
| Question to ask any probiotic manufacturer | Why it tells you something real |
|---|---|
| What is the full strain identifier of every organism in this product? | Without identifiers, there is no link to any published trial |
| What published trials use exactly this strain in a population close to mine? | Distinguishes evidence-backed strains from marketing-only blends |
| What lot testing do you run, and can I see a certificate of analysis? | Tests strain identity verification and contamination screening |
| What is the dose at end of shelf life, not just at manufacture? | Catches CFU declines that make a label number meaningless |
| What temperature and storage conditions preserve potency? | Reveals whether the product can survive a typical home or kennel environment |
| Who signs off on quality, and how can I reach them? | A real quality system has a name and a contact behind it |
If you want the one-page version to pin to your wall, the Probiotics for Newborn Puppies and Kittens Practice Update Card condenses what changed in the last 5 years, what the evidence says to do differently, and what to monitor next, with the citations behind each decision. Download it here.
Conclusion
Human neonatology has spent twenty years asking the right questions about probiotics and arriving at honest answers. The 2023 European position paper narrowed the field to a few named strains. The 2023 safety alert reframed quality and supervision as part of the safety story. Both lessons travel.
What does not travel are the strains, the doses, the regulatory frame, and the assumption of hospital-grade supervision. In many aspects, dog and cat newborns are not where human neonatology is.
That is the truth, and it should not embarrass anyone. Veterinary medicine is moving on this question.
Specific avenues, including dam and queen supplementation, peri-weaning support, post-antibiotic recovery, and strain-specific use around neonatal diarrhea, are visible on the horizon. They are not protocols yet, but they are the kind of avenues the human file tells us are worth exploring with care.
For breeders today, the most powerful import from the human neonatal world is not a product. It is a mindset: strain first, manufacturer second, conversation with your veterinarian third.
Bring observations, bring records, bring questions about specific strains. Your veterinarian is your neonatologist. Your records, exactly the ones described in the section above, are what make her job possible.
The whelping box and the queening box deserve the same discipline a neonatal unit brings to its smallest patients. Even, and especially, while the protocols for puppies and kittens are still being written.